

Epidemiology
- 25,000 ankle sprains each day in United States
- Up to 30% of outpatient sports medicine clinics
- Ankle injuries are the most common type of injury in high school athletes
Anatomy
- Lateral
- Lateral Collateral Complex
- Anterior talofibular ligament (most common)
- Calcaneofibular ligament (2nd most common)
- Posterior talofibular ligament
- Mechanism of Injury
- Inversions with either dorsiflexion or plantarflexion
- Lateral Collateral Complex

- Medial
- Deltoid Complex
- Posterior tibiotalar ligament
- Tibiocalcaneal ligament
- Tibionavicular ligament
- Anterior tibiotalar ligament
- Mechanism of Injury
- Forced eversion
- Deltoid Complex

- Syndesmotic (high ankle sprain)
- Distal Tibiofibular Syndesmosis
- Anterior-inferior tibiofibular ligament
- Posterior-inferior tibiofibular ligament
- Transverse tibiofibular ligament
- Interosseous membrane
- Interosseous ligament
- Inferior transverse ligament
- Mechanism of Injury
- External rotation with dorsiflexion
- Distal Tibiofibular Syndesmosis

Important History Questions
- What was the mechanism of injury?
- Could you walk immediately after the injury?
- Can you walk now?
- Any previous history of ankle injuries?
Physical Exam
- Observation
- Swelling or ecchymosis
- Ambulation to exam room
- Palpation
- Bony
- Entire fibula (from lateral malleolus to fibular head)
- Lateral malleolus
- 5th metatarsal
- Navicular
- Soft Tissue
- Palpate each ligament based on mechanism
- Special Maneuvers
- Lateral Injuries
- Anterior drawer
- Stabilize proximal leg to the ankle and grasp calcaneous and apply anterior force
-
- Talar tilt
- Stabilize proximal leg to ankle and grasp calcaneous and apply inversion force
-
- Anterior drawer
- Syndesmotic Injuries
- Squeeze test (Hopkin’s test)
- Compression of tibia and fibula at mid calf
-
- External rotation stress test (Kleiger’s test)
- Stabilize proximal leg to the ankle and applying external rotation force to the forefoot
-
- Squeeze test (Hopkin’s test)
- Lateral Injuries
- Bony
Grading and Classifications

Indications for Radiography
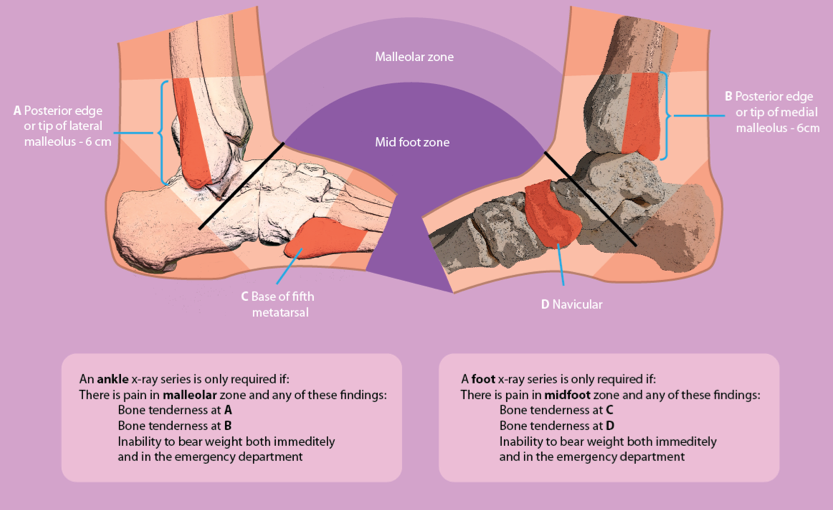
- Ottawa Rules of Foot and Ankle
- Published in 1996 and showed reduction of ankle x-rays by 28% if none of the following are present:
- Posterior lateral malleolar tenderness
- Posterior medial malleolar tenderness
- Base of 5th metatarsal tenderness
- Navicular tenderness
- Inability to ambulate both immediately and in the ED
- Published in 1996 and showed reduction of ankle x-rays by 28% if none of the following are present:
- Views
- Standard three views (AP, Lateral, Mortise)

- Varus stress view

- MRI
- Used for clinically suspicious of syndesmotic injury with normal radiographs

Management
- Orthopaedic Referral
- Fracture
- Dislocation/Subluxation
- Syndesmotic injury
- Tendon rupture
- Uncertain diagnosis
- Non-operative
- Low ankle
- RICE
- Cryotherapy 20 min every 2 hours for 48 hours
- May use crutches and NWB up to 10 days (Grade II and III)
- Early immobilization = better recovery
- Cast vs CAM Boot vs Aircast
- NSAIDs for pain control
- Refer to physical therapy for grade II and III for rehabilitation exercises
- RICE
- Syndesmotic
- CAM Boot vs short leg cast for 2-3 weeks
- Low ankle
- Operative
- Indications
- Low Ankle
- Any grade with continued pain and instability despite extensive non-operative management
- Any grade with bony avulsion
- Syndesmotic
- Instability on radiographs
- Continued pain despite conservative pain
- Associated ankle fracture
- Low Ankle
- Procedures
- Low Ankle
- Modified Brostrum
- Anatomic shortening and reinsertion of the ATFL and CFL
-
- Tendon transfer and tenodesis
-
- Modified Brostrum
- Syndesmotic
- Screw fixation
-
- Suture button
-
- Low Ankle
- Indications
Athlete Return to Play

Cottage Physician
References
- American College of Sports Medicine. Fact Sheets: Ankle Sprains. http://www.acsm.org/public-information/brochures-fact-sheets/fact-sheets. Accessed May 23, 2016.
- Wheeless’ Textbook of Orthopaedics. Ankle Sprain. http://www.wheelessonline.com/ortho/ankle_sprain. Accessed May 23, 2016.
- Low Ankle Sprain. http://www.orthobullets.com/foot-and-ankle/7028/low-ankle-sprain. Accessed May 23, 2016.
- High Ankle Sprain. http://www.orthobullets.com/foot-and-ankle/7029/high-ankle-sprain. Accessed May 23, 2016.
- Stiell I. Ottawa ankle rules. Can Fam Physician. 1996;42:478-80.
- Tiemstra JD. Update on Acute Ankle Sprains. Am Fam Physician. 2012;85(12):1170-1176.
- De Brucker Y, Jager T, Devos H, Boulet CG, Kichouh M, De Maeseneer M, Shahabpour M, de May J. Trauma mechanism in ankle fracture: Let’s do the twist. http://posterng.netkey.at/esr/viewing/index.php?module=viewing_poster&task=viewsection&pi=121495&ti=402298&searchkey=. Accessed May 24, 2016.
- Stress view of ankle – with deltoid ligament tear. http://radiopaedia.org/cases/stress-view-of-ankle-with-deltoid-ligament-tear. Accessed May 24, 2016.
- Hocutt JE, Jaffe R, Rylander CR, Beebe JK. Cryotherapy in ankle sprains. Am J Sports Med. 1982;10(5):316-9.
- Seah R, Mani-babu S. Managing ankle sprains in primary care: what is best practice? A systematic review of the last 10 years of evidence. Br Med Bull. 2011;97:105-35.
- Bleakley CM, O’connor SR, Tully MA, et al. Effect of accelerated rehabilitation on function after ankle sprain: randomised controlled trial. BMJ. 2010;340:c1964.
- Tsao LY. Radsource. High Ankle Sprain. http://radsource.us/high-ankle-sprains/. Accessed May 24, 2016.
