
***LISTEN TO THE PODCAST HERE***
Avascular Necrosis of The Hip
Epidemiology
- 200,000-300,000 estimated new cases each year in the United States
- Cause of approximately 10% of total hip replacements
- Mean age at time of diagnosis is < 50 years
Pathogenesis and Etiologies
Current thoughts on exact mechanisms are an area of hot debate, but include:
- Genetic predisposition
- Metabolic factors
- Vascular factors
- Vascular damage
- Increased intraosseous pressure
- Mechanical stresses
80% of all atraumatic cases of AVN are due to:
- Glucocorticoid Use
- Theories
- Microemboli in the arteries of the bone from alterations in lipid metabolism
- Increased bone marrow adipocyte size and number causing decreased venous outlow
- Changes venous endothelial cells of the bone leading to stasis and necrosis
- Dose of prednisone < 15-20 mg/day has lowest risk of developing AVN (<3%)
- Theories
- Alcohol Use
- Causes fat emboli, venous stasis, elevated cortisol, and adipocyte hyperrophy
- While not considered an absolute risk factor, it is associated with up to 31% of AVN cases
Trauma can also predispose patients to develop AVN and most commonly associated with:
- Femoral neck fracture
- Hip dislocations
Other atraumatic causes of AVN include sickle cell disease, Gaucher disease, decompression disease, treatment for ALL, and transplantation
Signs and Symptoms
- Pain
- Groin, thigh, and/or buttock pain
- Worse with weightbearing or motion
- Although 2/3rd may have rest pain
- 1/3rd may have night pain
- Decreased ROM with forced internal rotation and abduction
- Limp
Imaging
- Plain Radiographs
- May not see any changes early in disease course
- Progression of changes
- Decreased density –> sclerosis –> subchondral radiolucency (crescent sign) and collapse

- Magnetic Resonance Imaging
- Much more sensitive than plain films
- May see early changes undetectable on plain radiographs
- T1 – Signal low-density line differentiating healthy and ischemic bone
- T2 – Second high-density line showing hypervascular granulation
- May see early changes undetectable on plain radiographs

- Much more sensitive than plain films


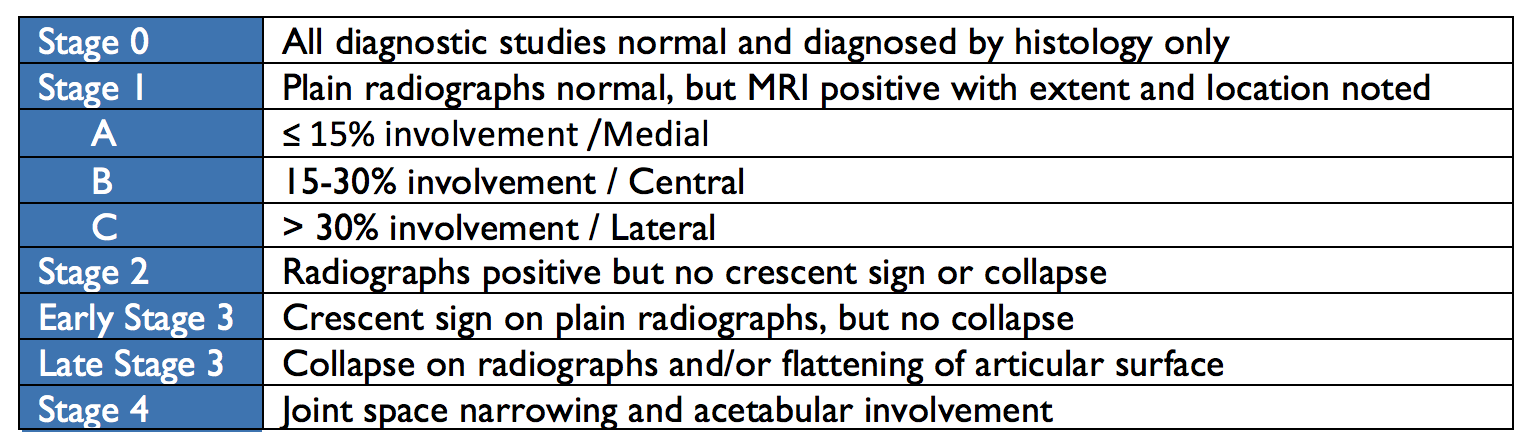
Classification and Staging
In 1993, The Association of Research Circulation Osseous (ARCO) staging system for AVN was developed to unify descriptions for treatment and research purposes.
Treatment
The goal of treatment is to preserve the native joint for as long as possible.
- Nonoperative Management
- Generally ineffective at halting the process
- Includes bed rest, partial weightbearing, and pharmacotherapeutics
- Bisphosphonates
- Slows bone resorption
- Vasodilators
- Decrease intraosseous pressure and improve blow flow
- Statins
- Anticoagulants
- Bisphosphonates
- Joint-Preserving Procedures
- Core Decompression
- Drills holes into femoral neck decrease pressure and allow for neovascularization

- http://www.ibji.com/education/patient-information/hip-pelvis/Core-Decompression-Avascular-Necrosis#vm_A_16a25645
- Vascularized Fibular Graft
- Larger core decompression with bone graft placed

- Core Decompression
- Total Joint Replacement
-


Slipped Capital Femoral Epiphysis (SCFE)
Definition
- Displacement of the capital femoral epiphysis from the neck of the femur through the physeal plate anterolaterally and superiorly

Risk Factors
- Obesity is #1 risk factor
- > 60% of patients in > 90th percentile for weight
- Renal failure
- History of radiation therapy
- Endocrine abnormalities
- Hypothyroidism, GH deficiency
Signs and Symptoms
The most common clinical presentation of SCFE are pain and altered gait, but can be divided into four presentation patterns:
- Preslip
- (+) pain, but no radiographical displacement of epiphysis
- May show widening of the physis
- Acute
- < 3 weeks duration
- (+) joint effusion but no metaphyseal remodeling
- 10-15% of initially presentation of hip pain and often associated with trauma
- Acute-on-chronic
- Worsening symptoms in known SCFE
- Chronic
- Most common pattern of presentation
- Vague, intermittent symptoms > 3 weeks
- (+) metaphyseal remodeling but no effusion
Pain is classically characterized as dull, aching in the hip, groin, thigh, or knee. Physical exam reveals decreased internal rotation and abduction ROM with increased pain. Passively flexing the affected hip while the leg is extended will cause external rotation and abduction.
Stability
- Stable Slips
- Walking and weightbearing still possible with or without crutches
- Unstable Slips
- No ability to weightbear, even with crutches
- No examination of the ROM of the hip should occur until orthopaedic consultation
Radiographic Evaluation
Most SCFE are diagnosed by plain radiography and have characteristic findings on each view:
- AP view
- Mild, widening, lucency, and irregularity of the physis
- Blurring of the junction between metaphysis and growth plate
- Klein’s Line
- Normal = intersecting lateral portion of femoral head from superior femoral neck
- SCFE = line passes outside of epiphysis

- Lateral View
- Usually obtained via frog-leg or cross-table
- Unstable SCFE should have true lateral
- Posterior displacements are best seen on lateral views
- Usually obtained via frog-leg or cross-table

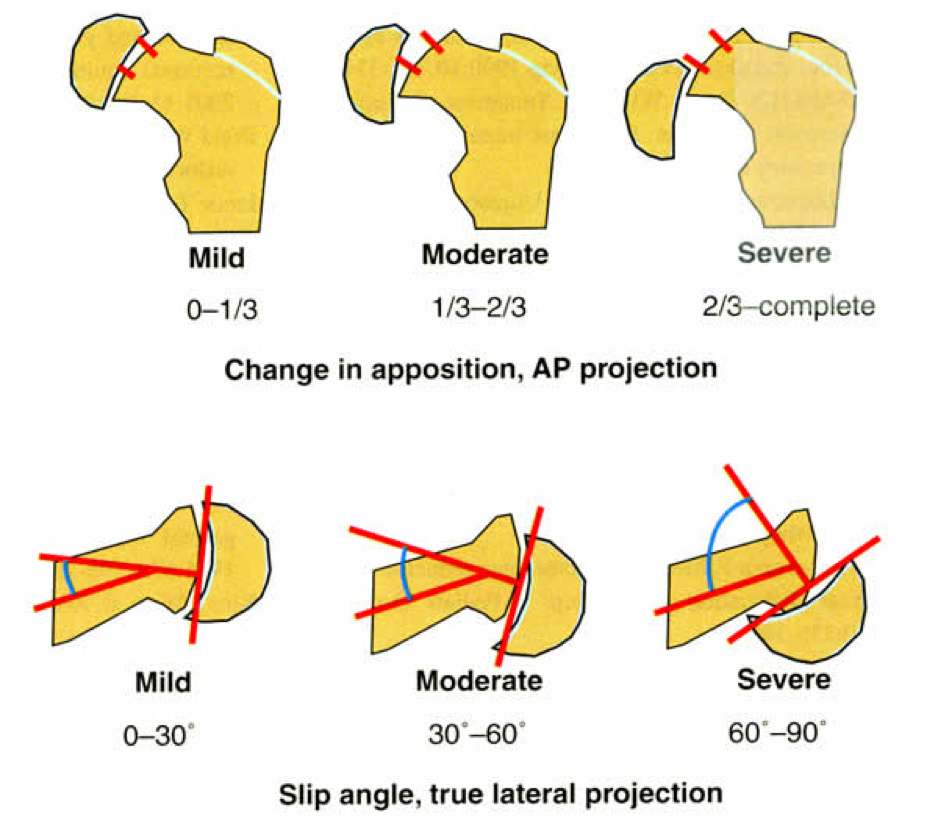
Grading of Severity
2 ways to grade severity: Displacement of femoral neck or Angle of Southwick.
- Displacement
- Mild = < 1/3rd the diameter of the femoral neck
- Moderate = > 1/3rd, but < 2/3rd the diameter of the femoral neck
- Severe = > 2/3rd the diameter of the femoral neck
- Angle of Southwick
- Mild = < 30o
- Moderate = 30-60o
- Severe = > 60o
Treatment
All SCFEs must be repaired surgically and the goals of surgery are to stabilize the diseased physis to prevent further slippage and avoid complications (AVN). Treatment of choice is a single cannulated screw placed in the center of the epiphysis.
References
- Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World Journal of Orthopedics. 2015; 6(8):590-601. [pubmed]
- Mankin HJ. Nontraumatic necrosis of bone (osteonecrosis). The New England journal of medicine. 1992; 326(22):1473-9. [pubmed]
- Jones JP. Fat embolism and osteonecrosis. The Orthopedic clinics of North America. 1985; 16(4):595-633. [pubmed]
- Dilisio MF. Osteonecrosis following short-term, low-dose oral corticosteroids: a population-based study of 24 million patients. Orthopedics. 2014; 37(7):e631-6. [pubmed]
- Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, Hirota Y. Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clinical orthopaedics and related research. 2010; 468(10):2715-24. [pubmed]
- Shigemura T, Nakamura J, Kishida S. The incidence of alcohol-associated osteonecrosis of the knee is lower than the incidence of steroid-associated osteonecrosis of the knee: an MRI study. Rheumatology (Oxford, England). 2012; 51(4):701-6. [pubmed]
- Slobogean GP, Sprague SA, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury. 2015; 46(3):484-91. [pubmed]
- LaPorte DM, Mont MA, Mohan V, Jones LC, Hungerford DS. Multifocal osteonecrosis. The Journal of rheumatology. 1998; 25(10):1968-74. [pubmed]
- Mont MA, Hungerford DS. Non-traumatic avascular necrosis of the femoral head. The Journal of bone and joint surgery. American volume. 1995; 77(3):459-74. [pubmed]
- ARCO Staging System. http://arco-intl.org/Newsletters/Gardeniers-1993-5-2/Gardeniers-1993.htm
- Loder RT. The demographics of slipped capital femoral epiphysis. An international multicenter study. Clinical orthopaedics and related research. 1996; [pubmed]
- Benson EC, Miller M, Bosch P, Szalay EA. A new look at the incidence of slipped capital femoral epiphysis in new Mexico. Journal of pediatric orthopedics. 2008; 28(5):529-33. [pubmed]
- Murray AW, Wilson NI. Changing incidence of slipped capital femoral epiphysis: a relationship with obesity? The Journal of bone and joint surgery. British volume. 2008; 90(1):92-4. [pubmed]
- Koop S, Quanbeck D. Three common causes of childhood hip pain. Pediatric clinics of North America. 1996; 43(5):1053-66. [pubmed]
- Causey AL, Smith ER, Donaldson JJ, Kendig RJ, Fisher LC. Missed slipped capital femoral epiphysis: illustrative cases and a review. The Journal of emergency medicine. 1995; 13(2):175-89. [pubmed]
- Reynolds RA. Diagnosis and treatment of slipped capital femoral epiphysis. Current opinion in pediatrics. 1999; 11(1):80-3. [pubmed]
