PAINE PANCE Postcard – Hand Foot Mouth Disease Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Lead Poisoning Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
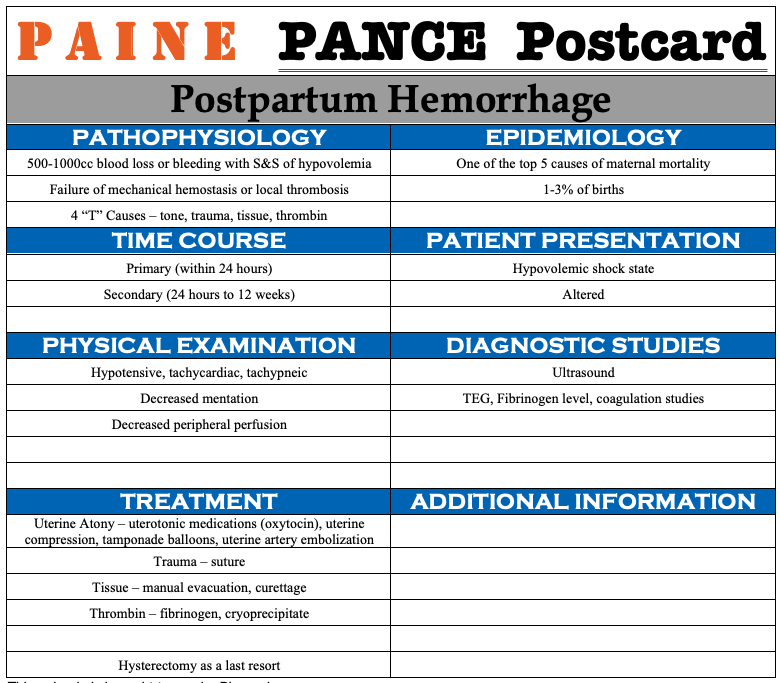
PAINE PANCE Postcard – Postpartum Hemorrhage Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Ovarian Torsion Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Bladder Prolapse (Cystocele) Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Pyelonephritis Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Pectus Carinatum Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
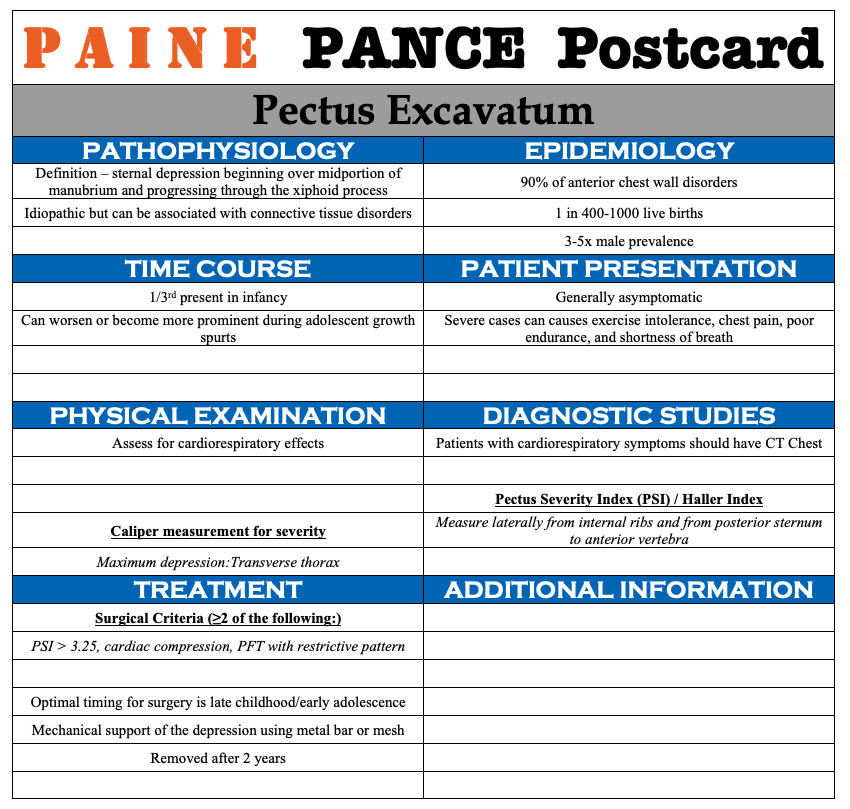
PAINE PANCE Postcard – Pectus Excavatum Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Septic Arthritis Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***