
***LISTEN TO THE PODCAST HERE***
Epidemiology
Adenovirus
- Viral (most common)
- Adenovirus (most common)
- Influenza
- Enterovirus
- Ebstein-Barr (EBV)
- Cytomegalovirus (CMV)
- Bacterial

Streptococcus pyogenes
- Group A streptococcus (GAS) (most common)
- Streptococcus pyogenes
- Mycoplasma pneumoniae
- Neisseria gonorrhoeae
- Corynebacteriium diptheriae
- Fusobacterium necrophorum (Lemierre Syndrome)
- Group A streptococcus (GAS) (most common)

History
- Several important historical factors that help differentiate viral from bacterial causes
- Immunization status
- Timing
- Viral – slower onset
- Bacterial – abrupt onset
- Fever
- Viral – afebrile to high-normal temperature
- Bacterial – tend to be > 100.4oF (38oC)
- Respiratory Complaints
- Viral – cough is common
- Bacterial – cough is often absent
- Dyspnea – suggests serious causes (see below)
- Fatigue
- Can occur in both viral and bacterial, but if prolonged may suggests EBV
- HEENT
- Viral – Coryza, ear pain, eye redness and watery drainage
- Bacterial – no associated complaints
- Hoarseness
- Viral – common
- Bacterial – worry about serious causes (see below)
- Drooling suggests impending airway collapse and is an emergency
- Rash
- Viral – macular with no texture
- Bacterial – scarlatiniform with “sand-paper”texture

Scarlatiniform Rash
- Neck pain or swelling
- Viral – generally negative, but EBV can cause tender lymphadenopathy
- Bacterial – lymphadenopathy common, investigate serious causes
Physical Exam
- Oropharynx
- Exudates
- Viral – Generally negative, but EBV can have
- Bacterial – hallmark of diagnosis
- Thick, pseudomembrane suggest diphtheria
- Exudates
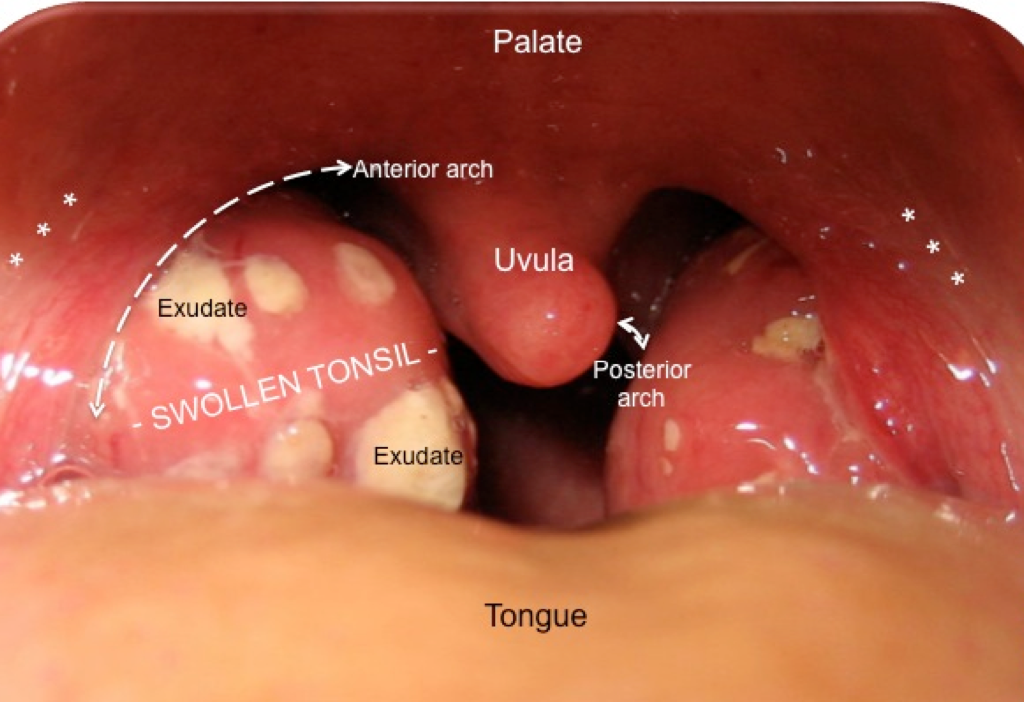
- Palate
- Both viral and bacterial can causes
- Classically associated with EBV and GAS
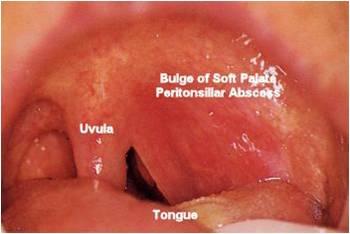
- Uvula
- Viral – may be edematous, but midline
- Bacterial – generally doesn’t affect it
- Deviation suggests peritonsillar abscess
- Neck
- Viral – generally no lymphadenopathy, except with EBV
- Bacterial – lymphadenopathy common
Pretest Considerations
- Centor Criteria
- Developed in 1981 to help in the clinical decision making of adults with strep throat in the emergency department
- 4 Variables
- Tonsillar exudates
- Swollen, tender anterior cervical lymphadenopathy
- Absence of cough
- History of fever
- Predicted the probability of being culture positive
- 0 – 2.5%
- 1 – 6.5%
- 2 – 15%
- 3 – 32%
- 4 – 56%
- 4 Variables
- Developed in 1981 to help in the clinical decision making of adults with strep throat in the emergency department
- McIsaac Score
- Developed in 1998 and further stratified patients based on age
- 3-14 years (highest risk)
- 15-44 years
- > 45 years (negative risk)
- Developed in 1998 and further stratified patients based on age
- Modified Centor Criteria (Centor + McIsaac) (MD Calc)
- Variables
- Age Range
- 3-14 years (+1)
- 15-44 years (0)
- ≥ 45 years (-1)
- Exudate or swelling of tonsils (+1)
- Tender, swollen anterior cervical lymphadenopathy (+1)
- Temperature ≥ 38oC (+1)
- Absence of cough (+1)
- Age Range
- Probability of strep infection
- 1 point – 5-10%
- 2 points – 11-17%
- 3 points – 28-35%
- 4 or 5 points – 51-53%
- Testing recommendations
- No testing if 0 or 1 point
- Optional testing if 2 points
- Recommend testing if ≥ 3 points
- NO RECOMMENDATIONS FOR EMPIRIC TREATMENT
- Variables
Testing Options
- CAN NOT DIFFERENTIATE ACUTE INFECTION VS CHRONIC CARRIER
- Up to 21% of children 3-15yo are carriers

Beta-hemolysis
- Up to 21% of children 3-15yo are carriers
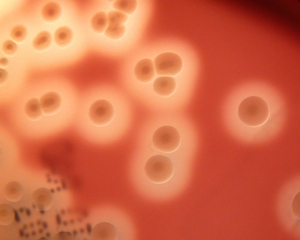
- Throat culture (gold standard)
- Sensitivity – 90-95%
- Testing for hemolysis on sheep blood agar
- May use RADT if results can’t be obtained in 48hr
- Rapid Antigen Detection Test (RADT)
- Sensitivity – 70-90%, but specificity – >95%
- Tests only for group A strep (S.pyogenes)
- Decision Pathway for Testing
- Modified Centor Criteria ≥ 4
- RADT due to high likelihood of positive culture
- If RADT negative, perform culture and wait 24hr results for treatment
- Modified Centor Criteria 2-3
- Perform throat culture and wait 24hr results for treatment
- Modified Centor Criteria ≤ 1
- No testing required
- Modified Centor Criteria ≥ 4
Special Testing Considerations
- Suspect infectious mononucleosis:
- Often have similar findings to bacterial infections with posterior lymphadenopathy and negative RADT and negative culture
- Morbilliform rash after starting amoxicillin or ampicillin

-
- CBC may show lymphocytic predominance
- Rapid heterophile antibody test (Monospot)
- Only positive after 2 weeks of illness
- EBV serology (IgM and IgG)
Serious Causes of Sore Throat
- Epiglottis
- High fever, toxic appearance, respiratory distress, tripod positioning, drooling
- Abscess
- Retropharyngeal
- Fever, neck pain, trismus, < 4yr
- Peritonsillar
- Deviated uvula, “hot potato voice”, adolescents, soft palate swelling
- Retropharyngeal
- Diptheria
- Unimmunized, recent travels to endemic country, gray-pseudomembrane
- Lemierre Syndrome
- Fusobacterium sp. or mixed anaerobes, toxic appearance, recent jugular line placement
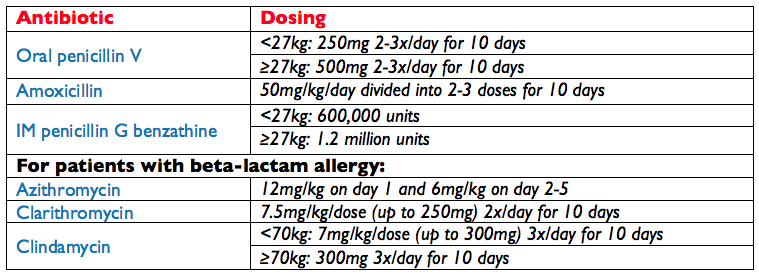
Treatment
Cottage Physician Reference
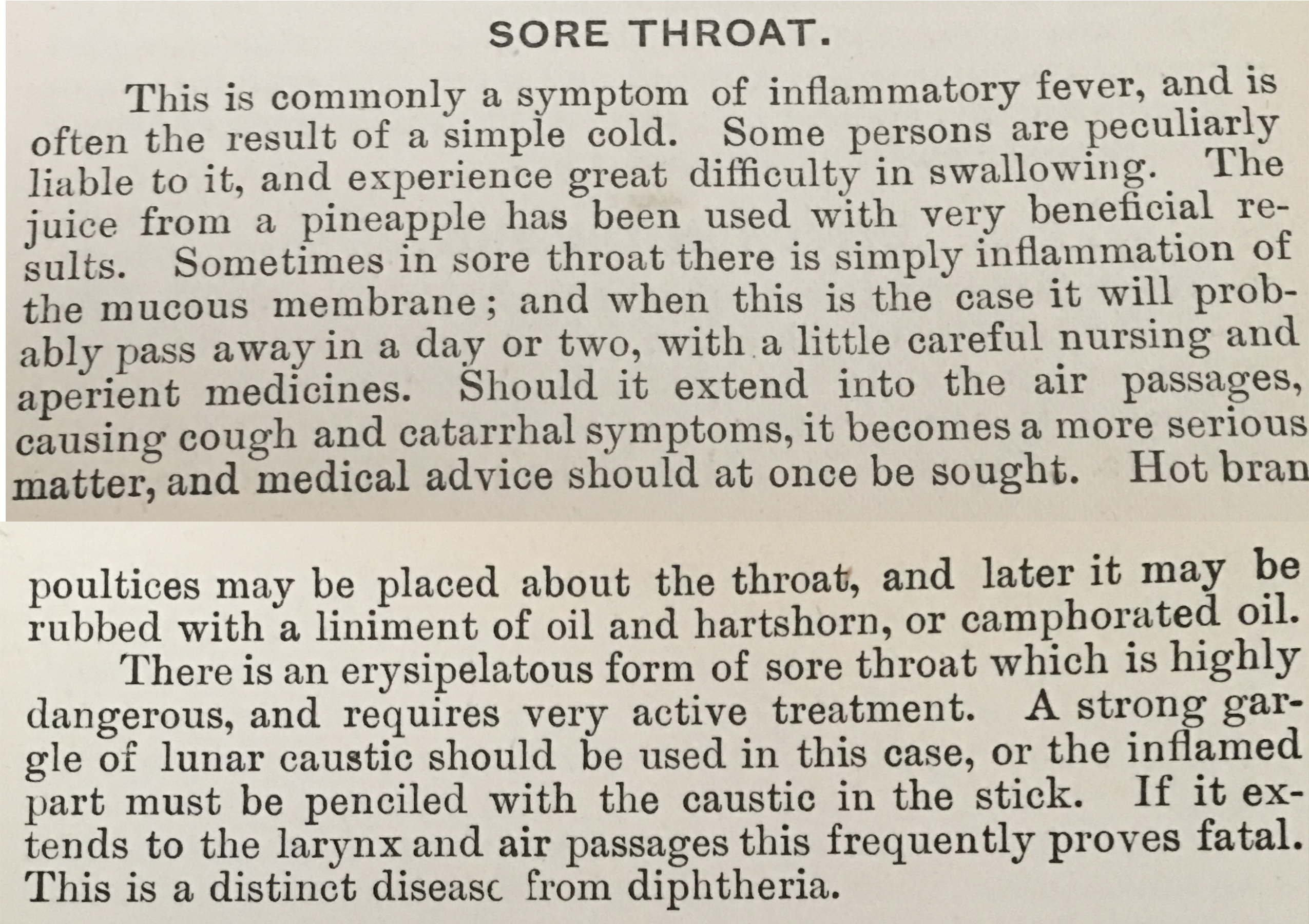
The Cottage Physician. 1893.
References
- Gerber MA. Diagnosis and treatment of pharyngitis in children. Pediatr Clin North Am. 2005;52(3):729-47, vi.
- Bisno AL. Acute pharyngitis. N Engl J Med. 2001;344(3):205-11.
- Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):e86-102.
- Centor RM, Witherspoon JM, Dalton HP, Brody CE, Link K. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1(3):239-46.
- Mcisaac WJ, White D, Tannenbaum D, Low DE. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ. 1998;158(1):75-83.
- Fine AM, Nizet V, Mandl KD. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med. 2012;172(11):847-52.
- Gerber MA. Comparison of throat cultures and rapid strep tests for diagnosis of streptococcal pharyngitis. Pediatr Infect Dis J. 1989;8(11):820-4.
- Shaikh N, Leonard E, Martin JM. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: a meta-analysis. Pediatrics. 2010;126(3):e557-64.
- Rafei K, Lichenstein R. Airway infectious disease emergencies. Pediatr Clin North Am. 2006;53(2):215-42.
- Page NC, Bauer EM, Lieu JE. Clinical features and treatment of retropharyngeal abscess in children. Otolaryngol Head Neck Surg. 2008;138(3):300-6.
- Goldenberg NA, Knapp-clevenger R, Hays T, Manco-johnson MJ. Lemierre’s and Lemierre’s-like syndromes in children: survival and thromboembolic outcomes. Pediatrics. 2005;116(4):e543-8.
- American Academy of Pediatrics. Group A Streptococcal Infections. In: Red Book: 2015 Report of the Committee on Infectious Diseases, 30th, Kimberlin DW, Brady MT, Jackson MA, Long SS (Eds), American Academy of Pediatrics, Elk Grove Village, IL 2015. p.732.
