*** LISTEN TO THE PODCAST HERE ***






















Question
A 3yo girl is brought to your office by her parents for concern of asthma. They state that when she plays with her siblings, she often gets short of breath and needs to stop to rest for a few minutes. She is otherwise healthy and was born at 38 weeks gestation via cesarean section. She has had an uncomplicated past medical history and is up to date on all immunizations.
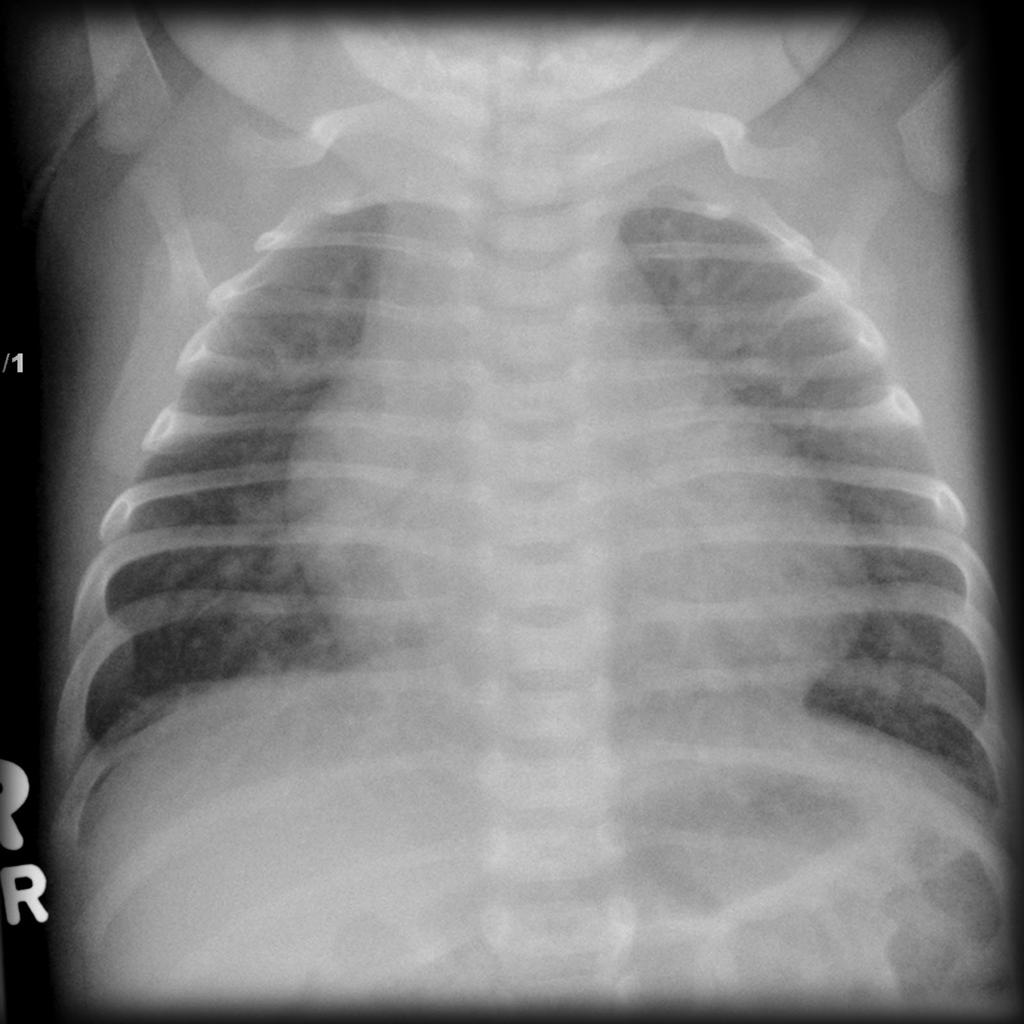
Physical examination reveals a well-nourished, well-developed girl, who is at 67% for height and 46% for weight for her age. Vital signs are BP-110/68, HR-87, RR-13, O2-100%, and temperature-98.7o. There is no evidence of cyanosis and auscultation findings are below.
Answer

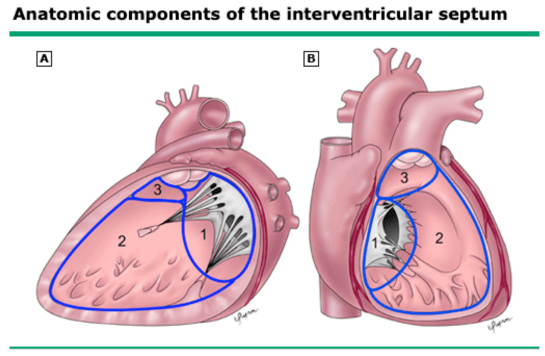
2. This type of murmur and the above clinical features are most likely due to a patent ductus arteriosus.
3. After a Doppler echocardiogram has been performed, surgery would be the next step to close this defect. Pharmacologic therapy does not work as well in older infants and children. Transcatheter closure would be the preferred option given the patient’s age.




Epidemiology
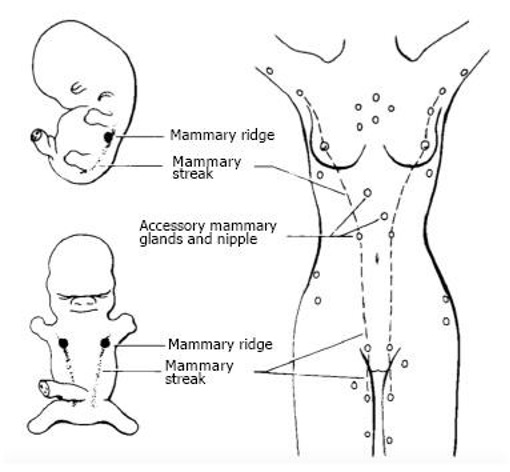
Normal Development
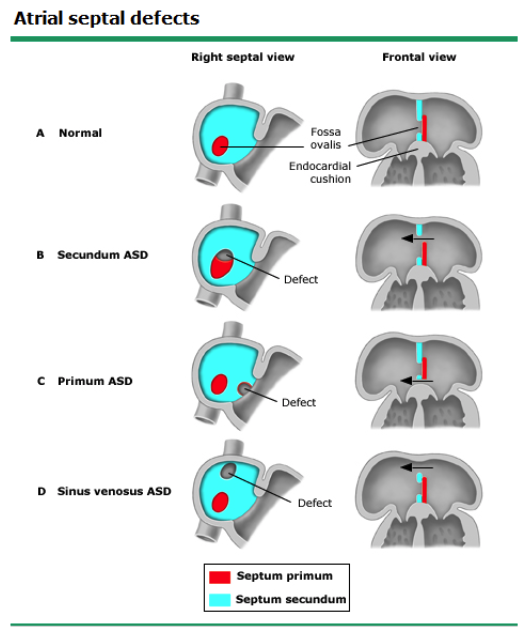
Types

Pathophysiology
Natural History
Clinical Presentation
Diagnostic Studies
Management

Epidemiology
Normal Development

Types
Natural History
Clinical Presentation
Diagnostic Studies
Management

Epidemiology
Normal Development
Types and Classifications


Pathophysiology
Clinical Presentation
Diagnostic Studies
Management


Epidemiology
Normal Development
Clinical Presentation
Diagnostic Studies
Management

Definition
Epidemiology
Pathogenesis
Pathophysiology
Clinical Manifestations
Diagnostic Studies



Management

Question
A 3yo girl is brought to your office by her parents for concern of asthma. They state that when she plays with her siblings, she often gets short of breath and needs to stop to rest for a few minutes. She is otherwise healthy and was born at 38 weeks gestation via cesarean section. She has had an uncomplicated past medical history and is up to date on all immunizations.
Physical examination reveals a well-nourished, well-developed girl, who is at 67% for height and 46% for weight for her age. Vital signs are BP-110/68, HR-87, RR-13, O2-100%, and temperature-98.7o. There is no evidence of cyanosis and auscultation findings are below.
Question
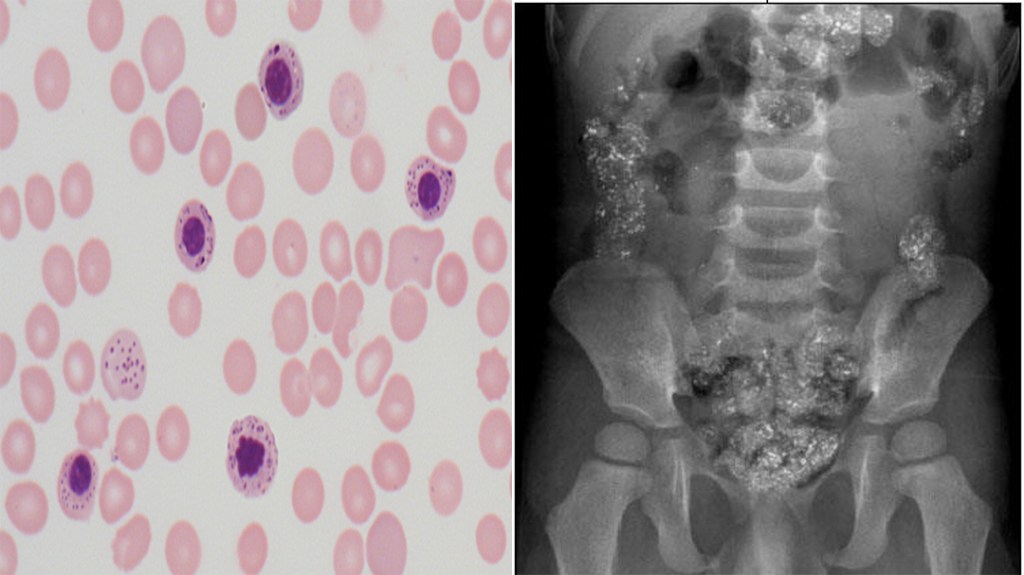
A 2yr old child is brought to the ED for altered mental status, vomiting, and lethargy. The parents states that this has been occurring since they moved into their grandmother’s home 2 months ago. Vitals signs are within normal limits and CBC reveals a hemoglobin – 10.1 mg/dL, mean corpuscular volume (MCV) – 71 fL/cell, and mean cell hemoglobin concentration (MCHC) – 29.1 g/dL. Peripheral smear and abdominal xray are below.
Answer


Question
A 2yr old child is brought to the ED for altered mental status, vomiting, and leathargy. The parents states that this has been occurring since they moved into their grandmother’s home 2 months ago. Vitals signs are within normal limits and CBC reveals a hemoglobin – 10.1 mg/dL, mean corpuscular volume (MCV) – 71 fL/cell, and mean cell hemoglobin concentration (MCHC) – 29.1 g/dL. Peripheral smear and abdominal xray are below.