
***LISTEN TO THE PODCAST HERE***
Epidemiology
- Estimated to be 50-80 per 100,000, or 240,000 per year
Definition
- Original
- Neurologic deficits lasting for < 24 hours
- Can still have permanent tissue injury
- Neurologic deficits lasting for < 24 hours

Ay H. Ann Neuro. 2005;57(5):679-86
- Consensus from American Heart Association and American Stroke Association
- Transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia WITHOUT acute infarction
- Benefits
- Tissue damage can be seen on imaging (more objective)
- Thus, encourages early neurodiagnostic tests
- Tissue damage can be seen on imaging (more objective)
Pathophysiology
- 3 main causes
- Intrinsic, vessel abnormality
- Atherosclerosis, lipohyalinosis, dissection, malformation, inflammation
- Embolic from distal source
- Inadequate cerebral blood flow
- Decreased perfusion pressure or increased blood viscosity
- Intrinsic, vessel abnormality
Classifications
- 3 main types
- Large artery, low-flow
- Brief (minutes to a few hours), recurrent, and sterotyped due to specific vessel it effects
- Often due to stenotic internal carotid, middle cerebral, or vertebral-basilar junction
- Brief (minutes to a few hours), recurrent, and sterotyped due to specific vessel it effects
- Embolic
- Discrete, infrequent, prolonged (several hours) episode
- Lacunar, small vessel
- Stenosis of intracerebral penetrating vessels from middle cerebral, basilar, or vertebral arteries
- HTN and DMII main culprits
- Large artery, low-flow
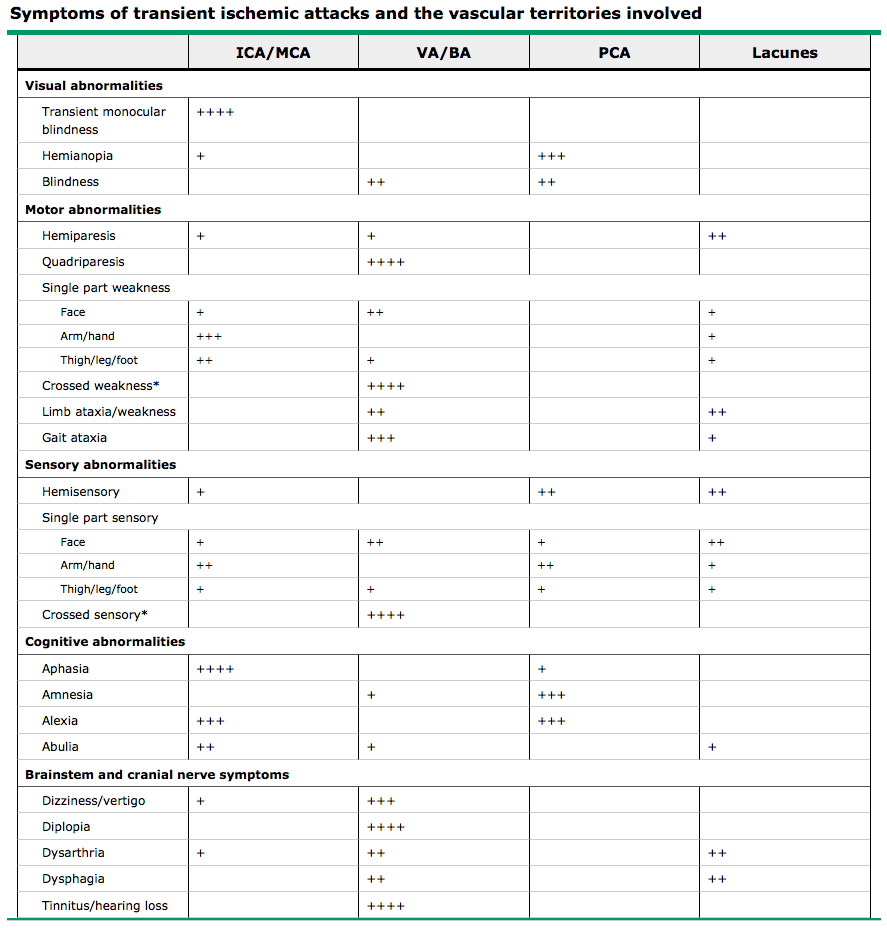
Signs and Symptoms
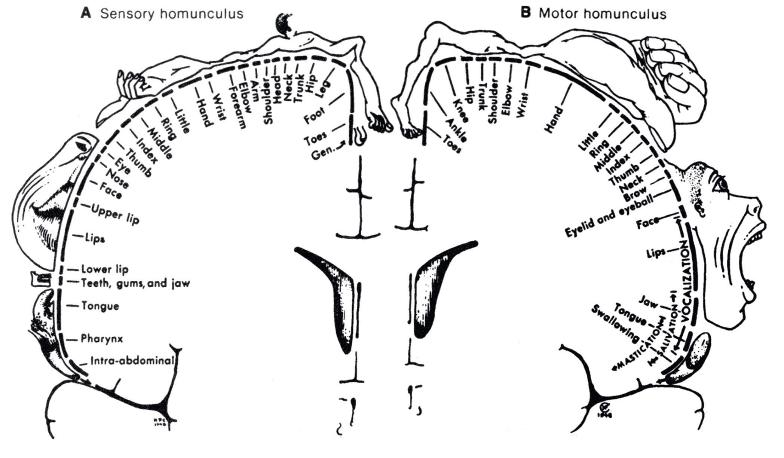
- All depends on the vessels being effected
- 2 Global Regions
- Anterior Circulation
- Internal carotid arteries
- Anterior cerebral artery (contralateral LE>UE weakness)
- Middle cerebral artery (contralateral face/UE>LE)
- Internal carotid arteries
- Posterior Circulation
- Vertebral arteries
- Basilar artery (crossed deficits, ataxis, visual disturbances)
- Cerebellar arteries (dizziness, N/V, visual disturbances)
- Posterior cerebral artery (visual disturbances, contralateral hemiplegia)
- Basilar artery (crossed deficits, ataxis, visual disturbances)
- Vertebral arteries
- Anterior Circulation
UpToDate
- Disabling symptoms that suggest stroke
- Complete hemianopsia
- Severe aphasia
- Visual/sensory extinction
- Any weakness limiting sustained effort against gravity
- NIHSS ≥ 5
- Inability to walk
- Modified Rankin Score ≥ 1
- Any deficit considered potentially disabling to patient or family
Stroke Mimics
- Seizures
- Migraine auras
- Syncope
- Peripheral vestibulopathies
- Pressure/position related peripheral neuropathies
- Metabolic derangements
- Hypo/hyperglycemia, renal, liver, pulmonary
Initial Evaluation
- Laboratory studies
- BMP, CBC, NH4, LFT, PT/PTT/INR
- EKG
- Brain imaging
- Preferred – Brain MRI with diffusion-weighted imaging
- Suboptimal – Non-contrast head CT
- CT perfusion scans becoming an option
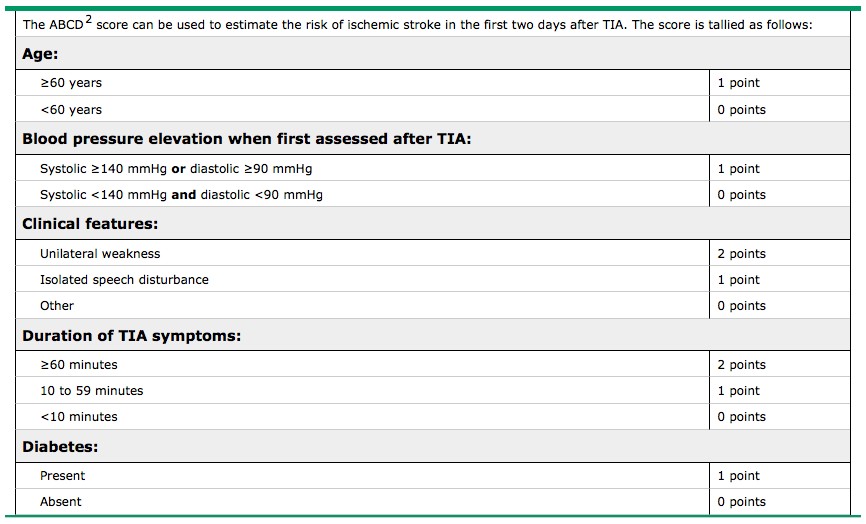
ABCD2 Score
- Used to estimate the risk of ischemic stroke in the first 48 hours after TIA
- 2-day stroke risk
- 0-3 – 1%
- 4-5 – 4%
- ≥ 6 – 8%
UpToDate
Admit or Outpatient???
- Recommend admission for:
- ABCD2 ≥ 3
- ABCD2 ≤ 2 and unsure if work-up can be completed in 48 hours as outpatient
- ABCD2 ≤ 2 and other evidence that this is caused by focal ischemia
Definitive Work-Up
- Neuroimaging within 24 hours of symptom onset
- Brain MRI with diffusion-weight imaging
- Neurovascular evaluation
- Preferred – 4-vessel catheter angiography
- Options – CTA, MRA, CDUS, TCD
- Cardiac Evaluation
- Reasonable to perform if neurovascular work-up is negative
- TTE if:
- Patient ≥ 45 years
- High suspicion of left ventricular thrombus
- TEE is contraindicated
- TEE preferred if:
- Patient < 45 years without history of CVD
- Patients with atrial fibrillation
- Patients with mechanical valve
- Patients with suspected aortic pathology
- High pretest probability of cardiac embolic source
UpToDate
Secondary Stroke Prevention
- Medical Management
- Hypertension
- Antiplatelet (ASA and clopidogrel)
- Statins (intensive therapy)
- Lifestyle modifications
- Large artery disease
- Carotid
- Revascularization
- Endarterectomy
- Stenting
- Revascularization
- Extracranial vertebral
- Angioplasty and stenting
- Intracranial cerebral vessels
- Intensive medical management
- Carotid
- Small artery disease
- Intensive medical management
- Cardiogenic embolism
- Atrial fibrillation
- Lifelong anticoagulation
- Myocardial infarction and left ventricular thrombus
- Anticoagulation for at least 3 months
- Mitral valve disease (prolapse, calcification)
- Antiplatelet
- Atrial fibrillation
Recent Study (video explanation)
One-Year Risk of Stroke after Transient Ischemic Attack or Minor Stroke (TIA Registry Investigators)
- 4789 patients, 61 sites in 21 countries
- Patients
- ≥ 18 years and had a TIA or minor stroke in the last 7 days
- Mean age – 66years
- 70% had HTN and DM
- 87% sought attention within 24 hours
- Modified Rankin scale ≤ 1
- ≥ 18 years and had a TIA or minor stroke in the last 7 days
- Timeline
- 2-day, 7-day, 30-day, 90-day, and 1-year (following for 5-years)
- Followed median 27.2 months
- Outcomes
- Primary (composite)
- Death from CV causes
- Nonfatal stroke
- Nonfatal ACS
- Secondary
- Individual components of primary
- TIA recurrence
- Death from any cause
- Bleeding
- Primary (composite)
- Results
- Primary
- 2% incidence of major fatal or nonfatal CV events
- Estimate of stroke risk was 5.1%
- Highest in 1st 90-days
- Patients with ABCD2 score ≤ 3 still had a 20% early recurrent stroke
- Higher ABCD2 score, large artery atherosclerosis, and multiple infarctions on imaging are strong independent predictors of recurrent events
- Risk of recurrent stroke was less than half of expected historical cohorts
- Attributed to faster and more aggressive secondary prevention
- Primary
Amarenco P. NEJM. 2016;374(16):1533-42
Cottage Physician
Cottage Physician – 1893
References
- Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics–2014 update: a report from the American Heart Association. Circulation. 2014;129(3):e28-e292.
- Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40(6):2276-93.
- Furie KL, Ay H. Initial evaluation and management of transient ischemic attacks and minor ischemic stroke. In: UpToDate. Waltham, MA.
- Ay H, Koroshetz WJ, Benner T, et al. Transient ischemic attack with infarction: a unique syndrome?. Ann Neurol. 2005;57(5):679-86.
- Quinn TJ, Dawson J, Walters MR, Lees KR. Reliability of the modified Rankin Scale: a systematic review. Stroke. 2009;40(10):3393-5.
- Levine SR, Khatri P, Broderick JP, et al. Review, historical context, and clarifications of the NINDS rt-PA stroke trials exclusion criteria: Part 1: rapidly improving stroke symptoms. Stroke. 2013;44(9):2500-5.
- Brott T, Adams HP, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989;20(7):864-70.
- Johnston SC, Rothwell PM, Nguyen-huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-92.
- Johnston SC, Nguyen-huynh MN, Schwarz ME, et al. National Stroke Association guidelines for the management of transient ischemic attacks. Ann Neurol. 2006;60(3):301-13.
- Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(7):2160-236.
- Whitlock RP, Sun JC, Fremes SE, Rubens FD, Teoh KH. Antithrombotic and thrombolytic therapy for valvular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e576S-600S.
- Amarenco P, Lavallée PC, Labreuche J, et al. One-Year Risk of Stroke after Transient Ischemic Attack or Minor Stroke. N Engl J Med. 2016;374(16):1533-42.

This iis a great post
LikeLike