*** LISTEN TO THE PODCAST HERE ***





Klumpke’s Palsy
Other Known Aliases – none
Definition – paralysis of the upper extremity from a lower trunk injury classically effecting C8-T1.
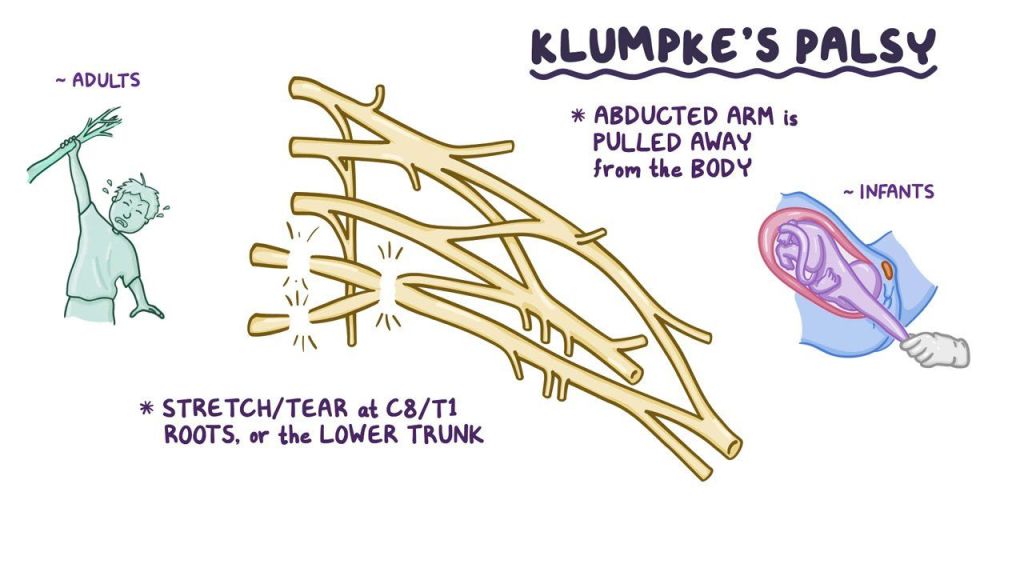
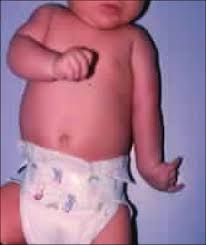
Clinical Significance – this brachial plexopathy can be infants as a result of birth trauma from pulling on an extending arm or in older children/adults from hanging from an outstretched arm. The classic manifestations are paralysis of the intrinsic hand muscles, fixed and flexed wrist and finger flexors, and sensory numbness of the C8/T1 dermatome leading to the textbook “claw hand” deformity.

History – Named after Augusta Déjerine-Klumpke (1859-1927), an American-born French physician who received her medical doctorate from the University of Paris in 1889 after becoming the first woman to be appointed interne des hôpitaux. She would immediately make a reputation for herself by being able to speak three languages and took an interest in neuroanatomy and physiology. She would meet fellow physician and future husband, Jules Dejerine, during her studies in medical school and the two would study and publish extensively together in the realm of neurology including the classic two-volume textbook on the anatomy of the nerve centers entitled “Anatomie des Centres Nerveux”. She would describe her eponymous condition in her 1885 case review of 18 patients taken from the available medical literature and would win her the Godard prize in 1886.


References











Question
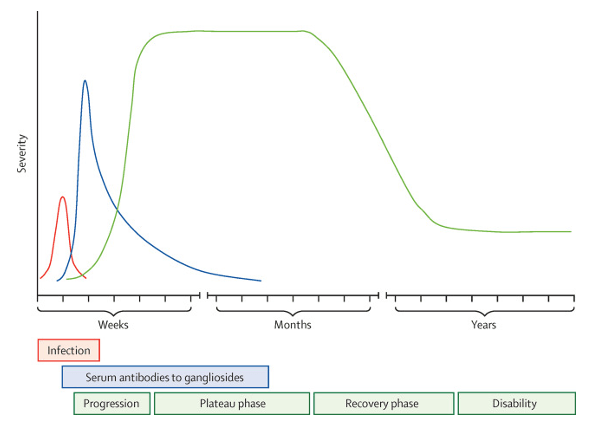
49yo man presents to his primary provider’s office with a 2-week history of bilateral leg weakness. He denies any pain associated with it and has never had any symptoms like this before. He denies any previous back problems and reports never remembers injuring his back. He thinks it first started in his feet when he noticed he was dragging is toes when walking, but now finds some difficulty lifting his legs when going up stairs. PMH is significant for hypertension (controlled on lisinopril) and osteoarthritis (controlled with exercise and celecoxib). He also reports having a pretty severe case of “food poisoning” a month ago when vacationing in the gulf, but is otherwise healthy.
Physical examination reveals 3/5 strength bilaterally with plantarflexion and dorsiflexion of the ankles and 4/5 strength bilaterally with hip and knee flexion. His ankle deep tendon reflex is absent and knee is diminished at 1+. Sensation and two-point discrimination of the feet are intact

Answer

Erb’s Palsy
Other Known Aliases – none
Definition – paralysis of the upper extremity from an upper trunk injury classically effecting C5-C6.

Clinical Significance – this brachial plexopathy is most commonly associated with birth trauma from a shoulder dystocia and depending on the severity of the injury, can resolve on its own or be permanent. The arm is classically internally rotated, with an extended and pronated forearm referred to as the “waiter’s tip” or “porter’s tip” sign.

History – Named after Wilhelm Heinrich Erb (1840-1921), a German neurologist who received his medical doctorate from the the University of Heidelberg in 1864. He would spend his early career assisting Nikolaus Friedreich and Ludwig von Buhl in Munich, before becoming chair of the pathology department at the University of Leipzig in 1880, and ultimately succeeding Friedreich in 1883. He is credited with popularizing the reflex hammer use in neurologic examinations and would be instrumental in identifying and describing myasthenia gravis, tabes dorsalis, and his eponymous point in the brachial plexus where this injury arises. Of note, he is also credited with the cardiac auscultation point where the S2 is best heard.

References

Question
49yo man presents to his primary provider’s office with a 2-week history of bilateral leg weakness. He denies any pain associated with it and has never had any symptoms like this before. He denies any previous back problems and reports never remembers injuring his back. He thinks it first started in his feet when he noticed he was dragging is toes when walking, but now finds some difficulty lifting his legs when going up stairs. PMH is significant for hypertension (controlled on lisinopril) and osteoarthritis (controlled with exercise and celecoxib). He also reports having a pretty severe case of “food poisoning” a month ago when vacationing in the gulf, but is otherwise healthy.
Physical examination reveals 3/5 strength bilaterally with plantarflexion and dorsiflexion of the ankles and 4/5 strength bilaterally with hip and knee flexion. His ankle deep tendon reflex is absent and knee is diminished at 1+. Sensation and two-point discrimination of the feet are intact
Question
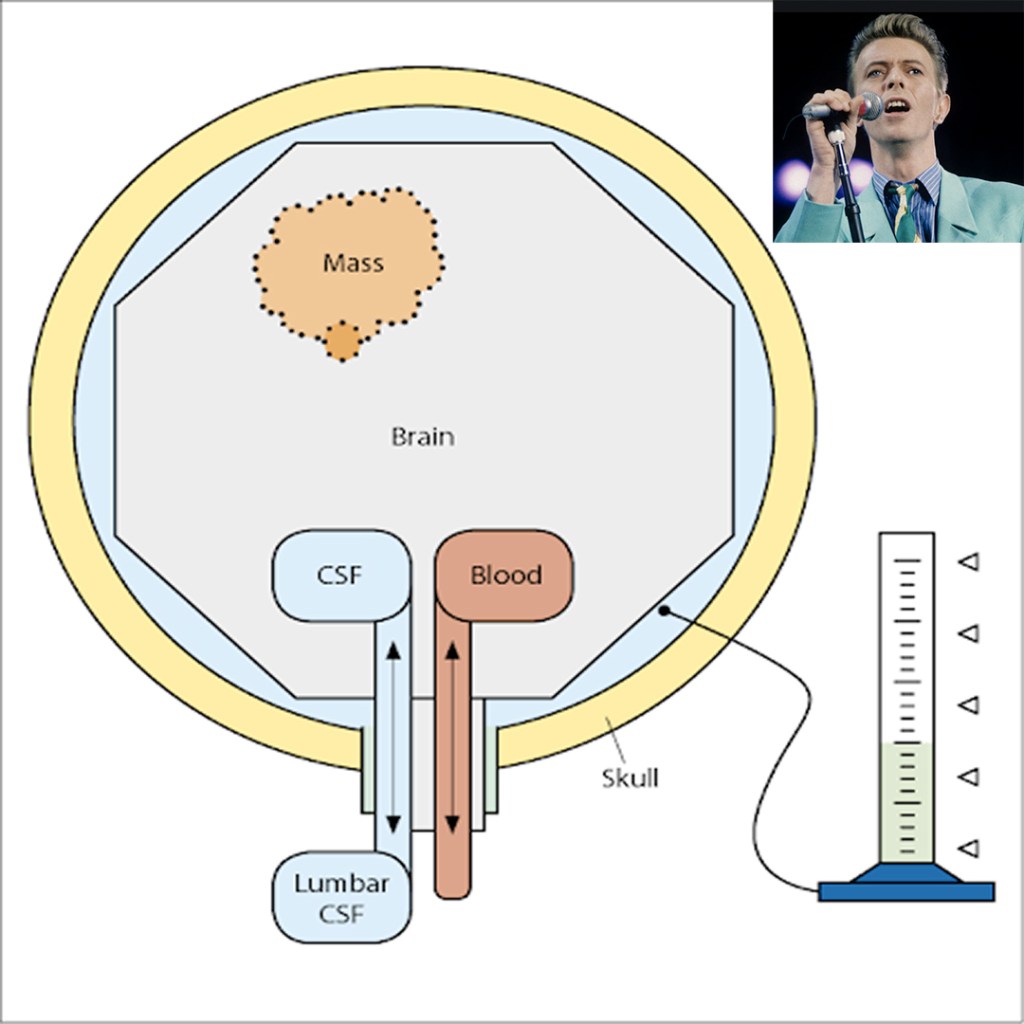
62yo man, with a history of pseudotumor cerebri, presents to your clinic with progressive headache and vision changes. You would like to confirm an increased intracranial pressure before sending him to the neurologist.
Answer
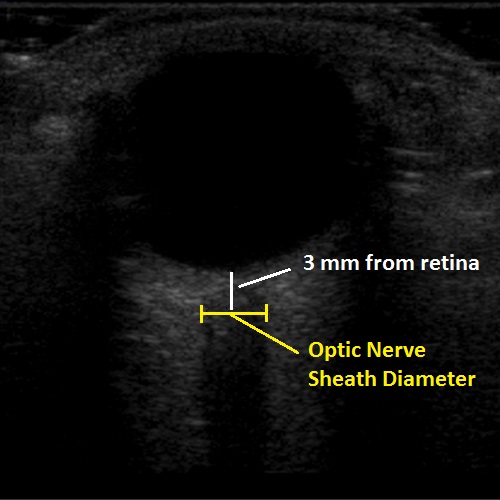
2. The new, hotness is using bedside POCUS to measure the optic nerve directly. Using the high frequency linear probe with a tegaderm placed over the patient eye, place a generous amount of gel over the globe and measure the optic nerve 3mm from the retina. A normal optic nerve should be < 5mm in diameter and anything over than suggests increased intracranial pressure

Question
62yo man, with a history of pseudotumor cerebri, presents to your clinic with progressive headache and vision changes. You would like to confirm an increased intracranial pressure before sending him to the neurologist.