

***LISTEN TO THE PODCAST HERE***
Definition and Cellular Physiology of Shock
The definition of shock is a clinical state of cellular and tissue hypoxia/perfusion due to:
- Reduced oxygen delivery
- Increased oxygen consumption
- Inadequate oxygen utilization
It basically comes down to the ratio between oxygen delivery (DO2) and oxygen extraction (VO2).
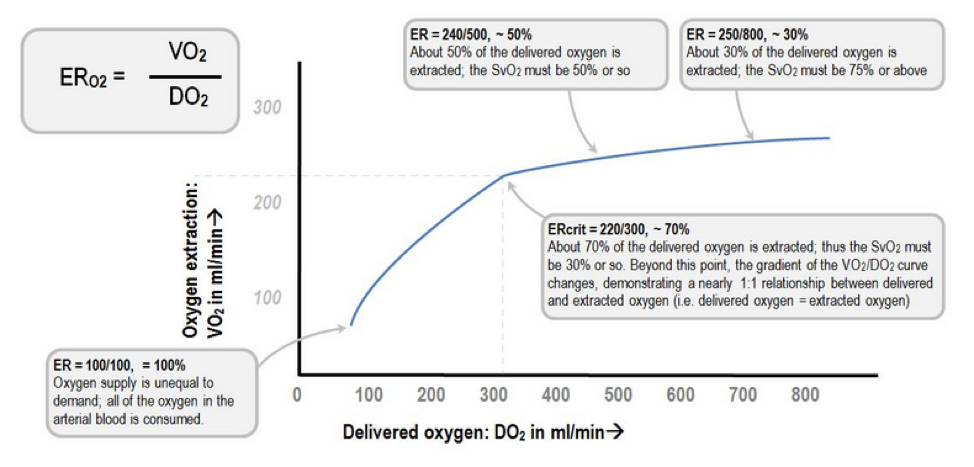
Extraction Ratio (ER)

Deranged Physiology

At the cellular level, shock hypoxemia causes cell membrane dysfunction leading to intracellular edema and leakage, as well inability to regulate cellular pH. This causes progressive acidemia, which in turn, have severe systemic effects on multiple organ systems.

Kherallah M.
Pathophysiology of Shock
BP = (HR x SV) x SVR
Factors effecting HR:
- Autonomic regulation
- Hormones
- Fitness levels
- Age
- Medications
Factors effecting SV:
- Preload
- Contractility
- Afterload
Factors effecting SVR:
- Vessel length
- Vessel diameter
- Blood viscosity
Signs and Symptoms of Shock
As perfusion decreases and hypoxia starts, the body begins to compensate and the signs and symptoms of shock are generally a result of this compensation.

Classifications and Causes of Shock

UpToDate
How to Diagnose Shock
Laboratory studies should be performed very early in the screening process for a patient with suspected shock as it will help you determine the degree of end organ perfusion. These include:
- Lactate (> 2 mmol/L)
- Creatinine
- LFTs
- ABG or VBG
There has been a tremendous amount of advancement in the diagnosis and management of patients in acute shock. For years, the pulmonary artery catheter was the gold standard for critically ill patients admitted to the ICU. It allowed for serial “measurements” of almost all the hemodynamic parameters you needed (PACWP, CO, CI, SVR, PAP, SvO2), but it was not without serious complications. It still has it’s place for certain disease management, but it is no longer indicated for diagnosing the different types of shock. I bring this up only because these parameters can be helpful when learning the different shock states as you can focus on 3 main variables: PACWP, CO/CI, and SVR.

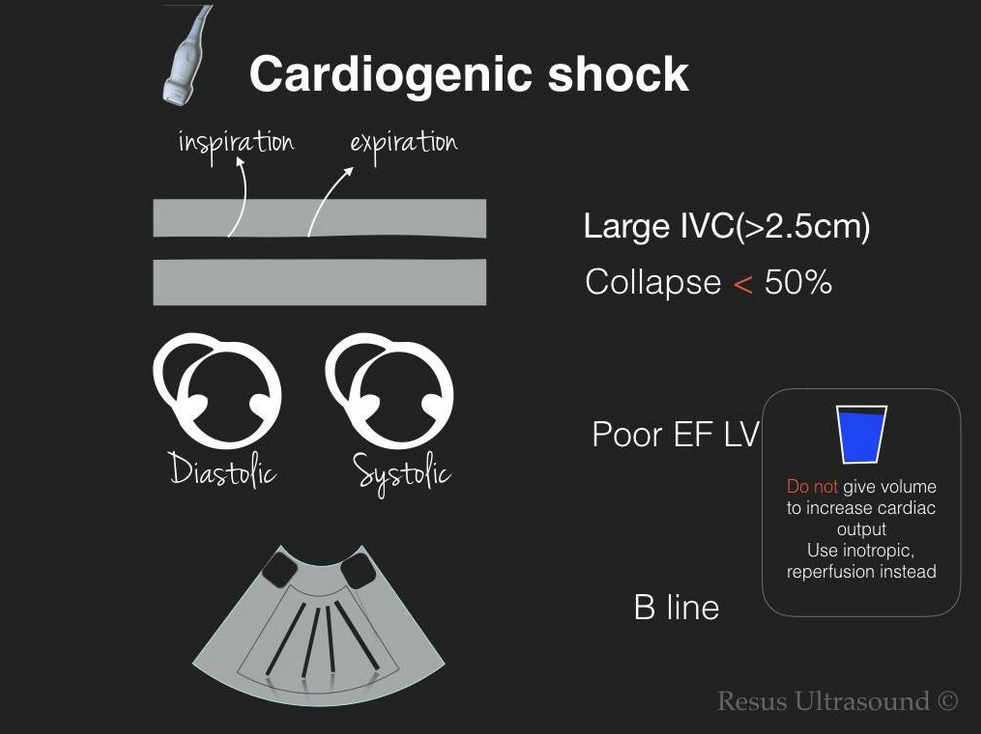
Point-of-Care ultrasonography (POCUS) has really become the test of choice for an undifferentiated shock patient, as it provides fast, vital information of the different causes of shock and allows for rapid rule-out of life-threatening conditions. There are several different types of POCUS algorithms used depending on the history and clinical context of the patient.

Rapid Ultrasound in Shock (RUSH) is used for undifferentiated patients. Scott Weingart does a great podcast on this technique here and Sinae EM Ultrasound did a step-by-step review here.

Another approach to undifferentiated shock is the Abdominal and Cardiac Evaluation with Sonography (ACES) protocol. It is used primarily in the UK and a good review can be found here.
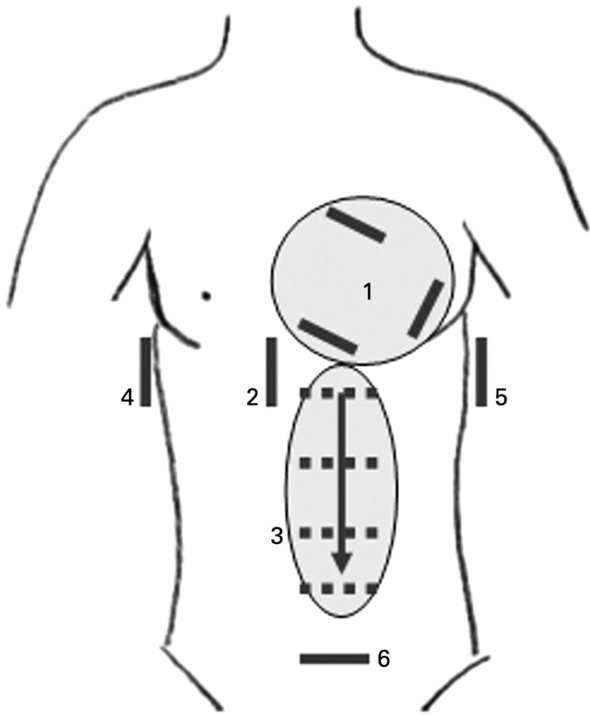
ACES Exam
Focus Assessed Transthoracic Echo (FATE) is a more detailed look at the heart to identify specific cardiac abnormalities.

If you have a trauma patient, you would use the Focused Assessment with Sonography for Trauma (FAST) exam to rapidly identify traumatic causes for hemorrhage and need for operative intervention.

FAST Exam
Really good paper in Critical Care that reviews echocardiography in shock management
http://ccforum.biomedcentral.com/articles/10.1186/s13054-016-1401-7
Management of Shock
Once you diagnose a patient with a specific type of shock, the management is pretty straight forward. If the patient is in hypovolemic, distributive, or obstructive shock, IV fluids should be used to improve perfusion and hemodynamics. The amount depends on the conditions, but usually starting with 1-2L of crystalloids is a good bet and then you can re-evaluate and repeat your ultrasound to look at the effects. If you have a trauma patient, then blood products should be started early on in the course until definitive control can be performed.
If adequate fluid resuscitation has not improved the hemodynamics or clinical picture, then pharmacologic agents are needed to improve perfusion. These can be broken down into vasopressors (increase vasomotor tone) and inotropes (increase contractility).
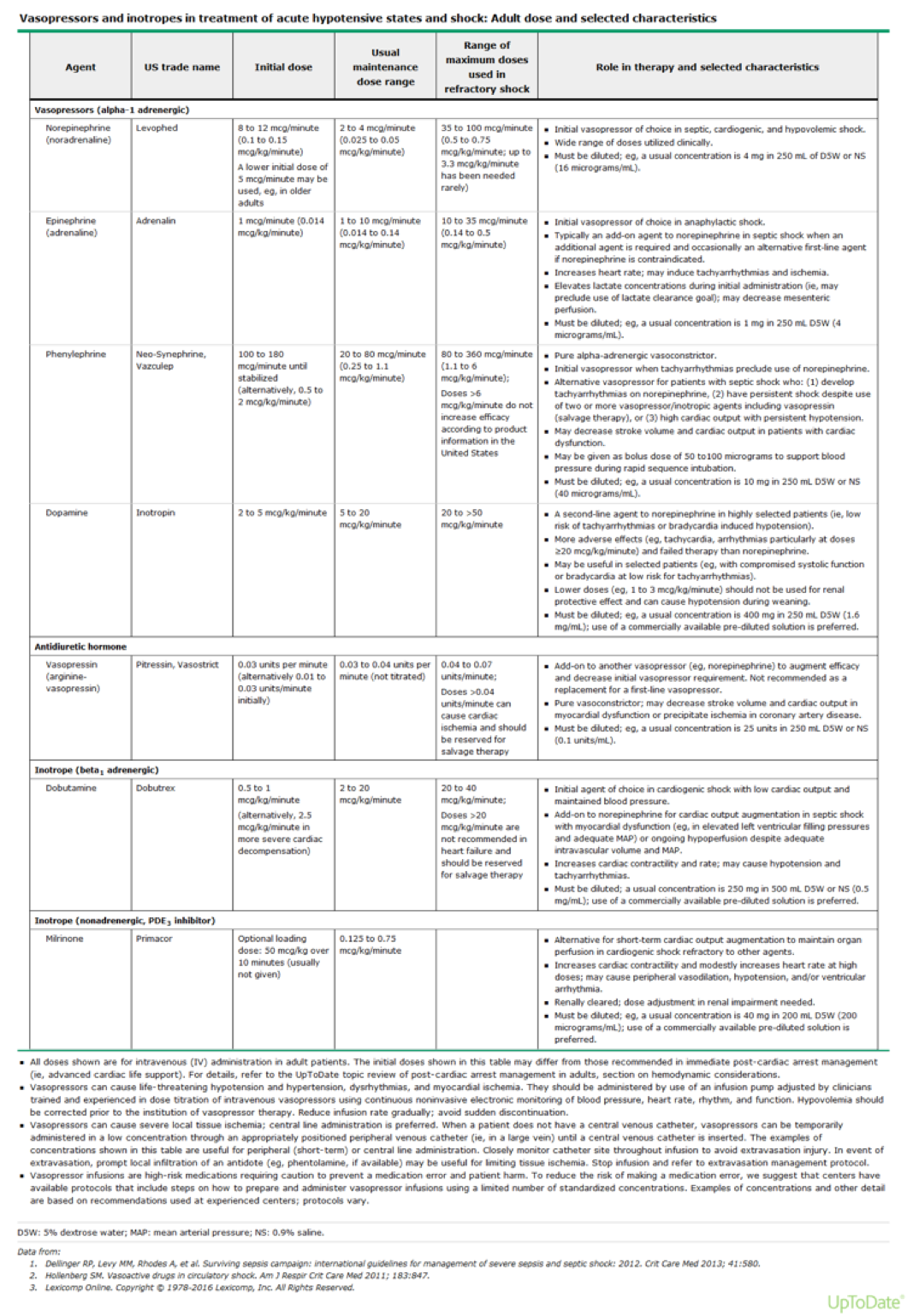
UpToDate



References
- Vincent JL, De Backer D. Circulatory shock. NEJM. 369(18):1726-34. 2013. [pubmed]
- Barber AE, Shires GT. Cell damage after shock. New horizons (Baltimore, Md.). 4(2):161-7. 1996. [pubmed]
- Deranged Physiology. The Relationship of Venous Oxygenation and Cellular Metabolism. Accessed 08/16/16. http://www.derangedphysiology.com/main/core-topics-intensive-care/arterial-blood-gas-interpretation/Chapter%208.0.1/relationship-venous-oxygenation-and-cellular-metabolism
- Kherallah M. Approach and Hemodynamic Evaluation of Shocks. Accessed 08/16/16. http://slideplayer.com/slide/3900131/
- Gaieski DF, Mikkelsen ME. Definition, classification, etiology, and pathophysiology of shcok in adults. In: UpToDate, Parsons PE (ed), UpToDate, Waltham, MA. Accesed 08/17/2016. http://www.uptodate.com/contents/definition-classification-etiology-and-pathophysiology-of-shock-in-adults?source=search_result&search=shock&selectedTitle=1%7E150#H18097167
- Shah MR, Hasselblad V, Stevenson LW. Impact of the pulmonary artery catheter in critically ill patients: meta-analysis of randomized clinical trials. JAMA. 294(13):1664-70. 2005. [pubmed]
- Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in Shock in the evaluation of the critically lll. Emergency medicine clinics of North America. 28(1):29-56, vii. 2010. [pubmed]
- Weingart SD, Duque D, Nelson B. EmCrit Blog. Rapid Ultrasound for Shock and Hypotension – the RUSH Exam. Accessed 08/17/16. http://emcrit.org/rush-exam/
- Labovitz AJ, Noble VE, Bierig M. Focused cardiac ultrasound in the emergent setting: a consensus statement of the American Society of Echocardiography and American College of Emergency Physicians. Journal of the American Society of Echocardiography. 23(12):1225-30. 2010. [pubmed]
- Atkinson PR, McAuley DJ, Kendall RJ. Abdominal and Cardiac Evaluation with Sonography in Shock (ACES): an approach by emergency physicians for the use of ultrasound in patients with undifferentiated hypotension. Emergency medicine journal : EMJ. 26(2):87-91. 2009. [pubmed]
- AIUM practice guideline for the performance of the focused assessment with sonography for trauma (FAST) examination. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 33(11):2047-56. 2014. [pubmed]
- Gaieski DF, Mikkelsen ME. Evaluation of and initial approach to the adult patient with undifferentiated hypotension and shock. In: UpToDate, Parsons PE (ed), Waltham, MA. Accessed on 08/17/16. http://www.uptodate.com/contents/evaluation-of-and-initial-approach-to-the-adult-patient-with-undifferentiated-hypotension-and-shock?source=see_link#H87905481

Pingback: Shock Related to Spinal Cord Injury – rathemblog
Great talk on shock. Love this sh**
LikeLike