*** LISTEN TO THE PODCAST HERE ***



Question
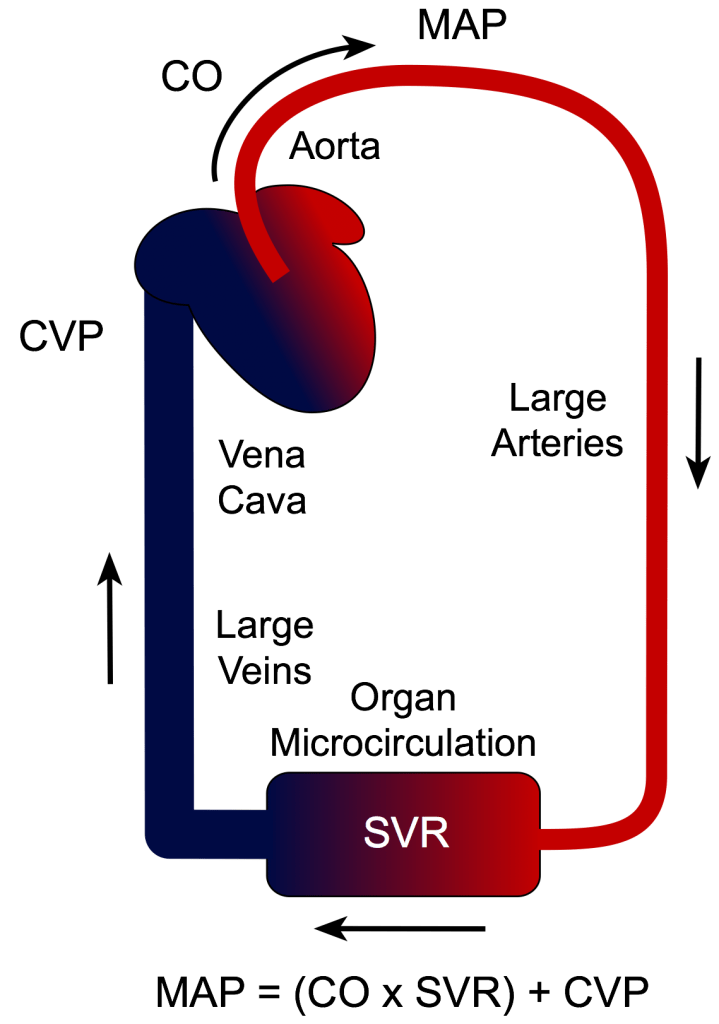
A large part of critical care and ICU management revolves around hemodynamic monitoring and support. But…..we typically don’t use traditional blood pressure (systolic and diastolic) numbers directly.
We use MAP!!!
Answer


References

Question
A large part of critical care and ICU management revolves around hemodynamic monitoring and support. But…..we typically don’t use traditional blood pressure (systolic and diastolic) numbers directly.
We use MAP!!!

Swan-Ganz Catheter
Other Known Aliases – pulmonary artery catheter
Definition – intravenous catheter that is maneuvered through the right side of the heart into the pulmonary artery.
Clinical Significance – This catheter can directly measure several important hemodynamic variables in critical illness:
It is “floated” through the right side of the heart using the flow of the blood to carry it into the pulmonary artery. This migration has a very characteristic pressure pattern to know where the catheter is in the vascular system.

History – Named after two physicians from Cedars-Sinai Medical Center, Jeremy Swan (1922-2005), an Irish American cardiologist, and William Ganz (1919-2009), a Slovak American cardiologist. Dr. Swan received his medical doctorate from Castleknock College and went on to become faculty at the Mayo Clinic before joining the faculty at Cedars-Sinai Hospital in Los Angeles. Dr. Ganz attended Charles University School of Medicine in Prague in 1938, but was closed in 1940 after the Nazi occupation of Czechoslovakia. Being jewish, he was then sent to a Hungarian Nazi labor camp and was actually scheduled to be sent to Auschwitz in 19944 before his escape. After hiding and waiting out the war, Dr. Ganz returned and graduated from Charles University in 1947 at the top of his class. He practiced in communist Czechslovakia until 1966 when he secretly defected to the US with his wife and sons. His first and only position as a physician in the US was at Cedars-Sinai Hospital, where he met Dr. Swan who got the idea of the catheter from watching the wind play with the sails of boats in the marina. Dr. Ganz had already published research on the use of thermodilution as a way to measure cardiac output and in 1970, they published their landmark article in the NEJM. It should be noted that German surgeon Werner Forssmann first demonstrated the safety of this type of catheter, by doing it on himself in 1929.


References
Osborn Wave
Other Known Aliases – J-wave, camel-hump, hypothermic hump
Definition – positive deflection occurring at the junction between the QRS complex and ST segment, commonly referred to as the J point
Clinical Significance – Osborn waves are classically seen in hypothermia with a core body temperature < 32°C (90°F), but also can be present in severe hypercalcemia, traumatic brain injury, and pericarditis. It is usually most prominent in the precordial leads.

History – Named after John J. Osborn (1917-2014), who was an American intensivist, and received his medical doctorate from Johns Hopkins University in 1943. He completed a nine-month residency in pediatrics before serving as an Army medical officer in World War II in the Pacific Theatre. He first published his preliminary animal research on hypothermia in 1943 before his military service, and picked it back up after returning stateside. He practiced from New York University to Stanford University and was a founding member of the Society of Critical Care Medicine. His research fostered the initial golden age of intensive care medicine and he worked on heart-lung machine designs, as well as hemodynamic monitoring devices. His eponymous paper was published in 1953 entitled “Experimental hypothermia; respiratory and blood pH changes in relation to cardiac function”


References

Wes Johnson, MSPAS, PA-C, (soon to be), DHSc was a former student of mine at UAB and was a respiratory therapist prior to PA school. He is the Regional Director of Clinical Education for Island Medical Management Emergency group in North Alabama. He won the Preceptor of The Year award from UAB in 2016 and currently finishing up his doctorate degree from A.T. Still University.
Twitter – @wesj2288
For the purposes of this podcast and post, we will be using the Puritan Bennett 840 ventilator (pictured below). All the term we use are synonymous with all vents, but the screens will be different.

Puritan Bennett 840


(For this section, refer back to the vent picture above)



Mode: AC
Vt: 6-8 mL/kg based on pt’s IBW
Rate: 12-16 bpm
FiO2: 100%
PEEP: 5.0
At the 5-minute mark:

This patient is ready for extubation. Everyone has their own magic numbers they want to see on the vent before they think about extubating a patient, but mine are:
These are basic principles and there are many variables that go into deciding to extubate a patient. LITFL does a great review here and goes through a very systematic approach.
Once this is all good, then you can perform a few bedside tests or measurements that can help predict success of extubation.

Prediction of Successful Extubation. The ICU Book.
Great post from Intensive Blog on “The Art and Science of Extubation”
References

Definition and Cellular Physiology of Shock
The definition of shock is a clinical state of cellular and tissue hypoxia/perfusion due to:
It basically comes down to the ratio between oxygen delivery (DO2) and oxygen extraction (VO2).
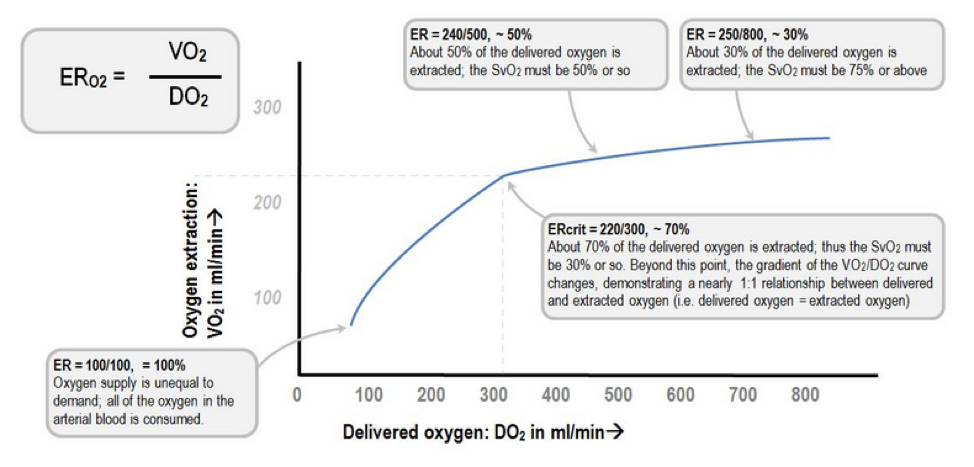
Extraction Ratio (ER)

Deranged Physiology

At the cellular level, shock hypoxemia causes cell membrane dysfunction leading to intracellular edema and leakage, as well inability to regulate cellular pH. This causes progressive acidemia, which in turn, have severe systemic effects on multiple organ systems.

Kherallah M.
Pathophysiology of Shock
BP = (HR x SV) x SVR
Factors effecting HR:
Factors effecting SV:
Factors effecting SVR:
Signs and Symptoms of Shock
As perfusion decreases and hypoxia starts, the body begins to compensate and the signs and symptoms of shock are generally a result of this compensation.

Classifications and Causes of Shock

UpToDate
How to Diagnose Shock
Laboratory studies should be performed very early in the screening process for a patient with suspected shock as it will help you determine the degree of end organ perfusion. These include:
There has been a tremendous amount of advancement in the diagnosis and management of patients in acute shock. For years, the pulmonary artery catheter was the gold standard for critically ill patients admitted to the ICU. It allowed for serial “measurements” of almost all the hemodynamic parameters you needed (PACWP, CO, CI, SVR, PAP, SvO2), but it was not without serious complications. It still has it’s place for certain disease management, but it is no longer indicated for diagnosing the different types of shock. I bring this up only because these parameters can be helpful when learning the different shock states as you can focus on 3 main variables: PACWP, CO/CI, and SVR.

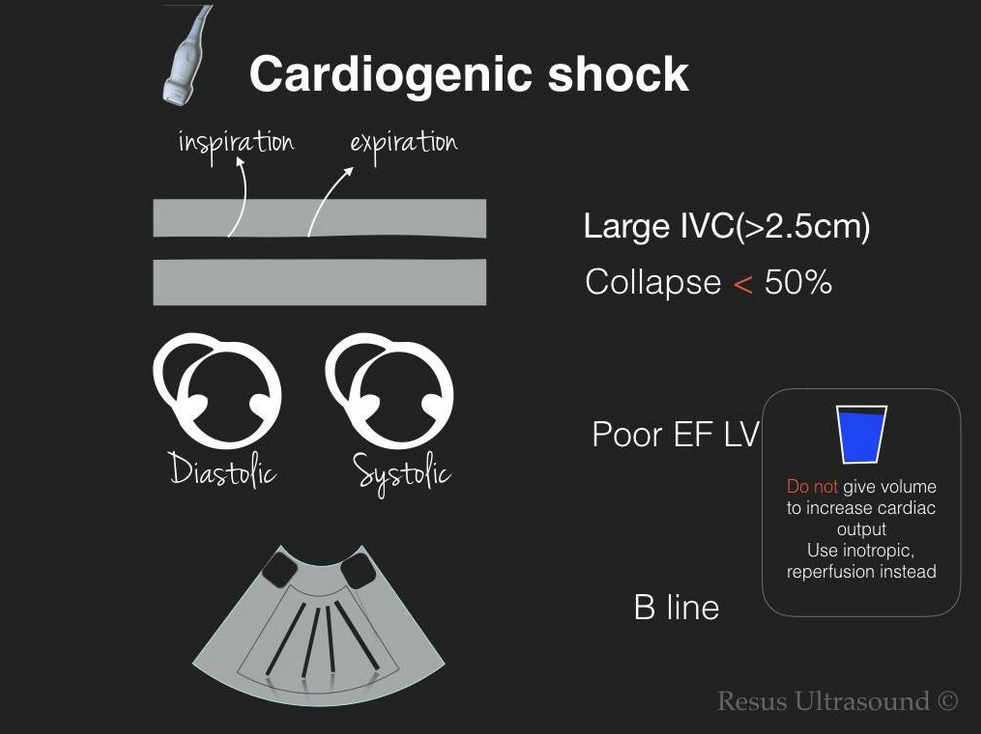
Point-of-Care ultrasonography (POCUS) has really become the test of choice for an undifferentiated shock patient, as it provides fast, vital information of the different causes of shock and allows for rapid rule-out of life-threatening conditions. There are several different types of POCUS algorithms used depending on the history and clinical context of the patient.

Rapid Ultrasound in Shock (RUSH) is used for undifferentiated patients. Scott Weingart does a great podcast on this technique here and Sinae EM Ultrasound did a step-by-step review here.

Another approach to undifferentiated shock is the Abdominal and Cardiac Evaluation with Sonography (ACES) protocol. It is used primarily in the UK and a good review can be found here.
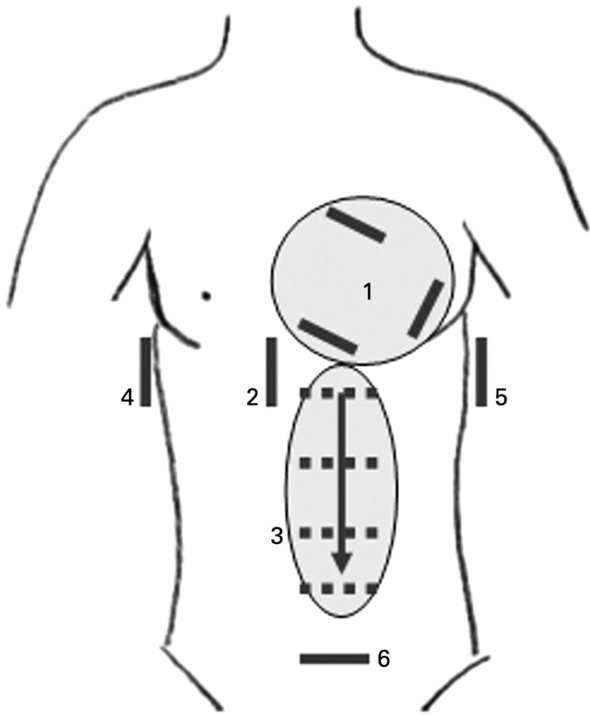
ACES Exam
Focus Assessed Transthoracic Echo (FATE) is a more detailed look at the heart to identify specific cardiac abnormalities.

If you have a trauma patient, you would use the Focused Assessment with Sonography for Trauma (FAST) exam to rapidly identify traumatic causes for hemorrhage and need for operative intervention.

FAST Exam
Really good paper in Critical Care that reviews echocardiography in shock management
http://ccforum.biomedcentral.com/articles/10.1186/s13054-016-1401-7
Management of Shock
Once you diagnose a patient with a specific type of shock, the management is pretty straight forward. If the patient is in hypovolemic, distributive, or obstructive shock, IV fluids should be used to improve perfusion and hemodynamics. The amount depends on the conditions, but usually starting with 1-2L of crystalloids is a good bet and then you can re-evaluate and repeat your ultrasound to look at the effects. If you have a trauma patient, then blood products should be started early on in the course until definitive control can be performed.
If adequate fluid resuscitation has not improved the hemodynamics or clinical picture, then pharmacologic agents are needed to improve perfusion. These can be broken down into vasopressors (increase vasomotor tone) and inotropes (increase contractility).
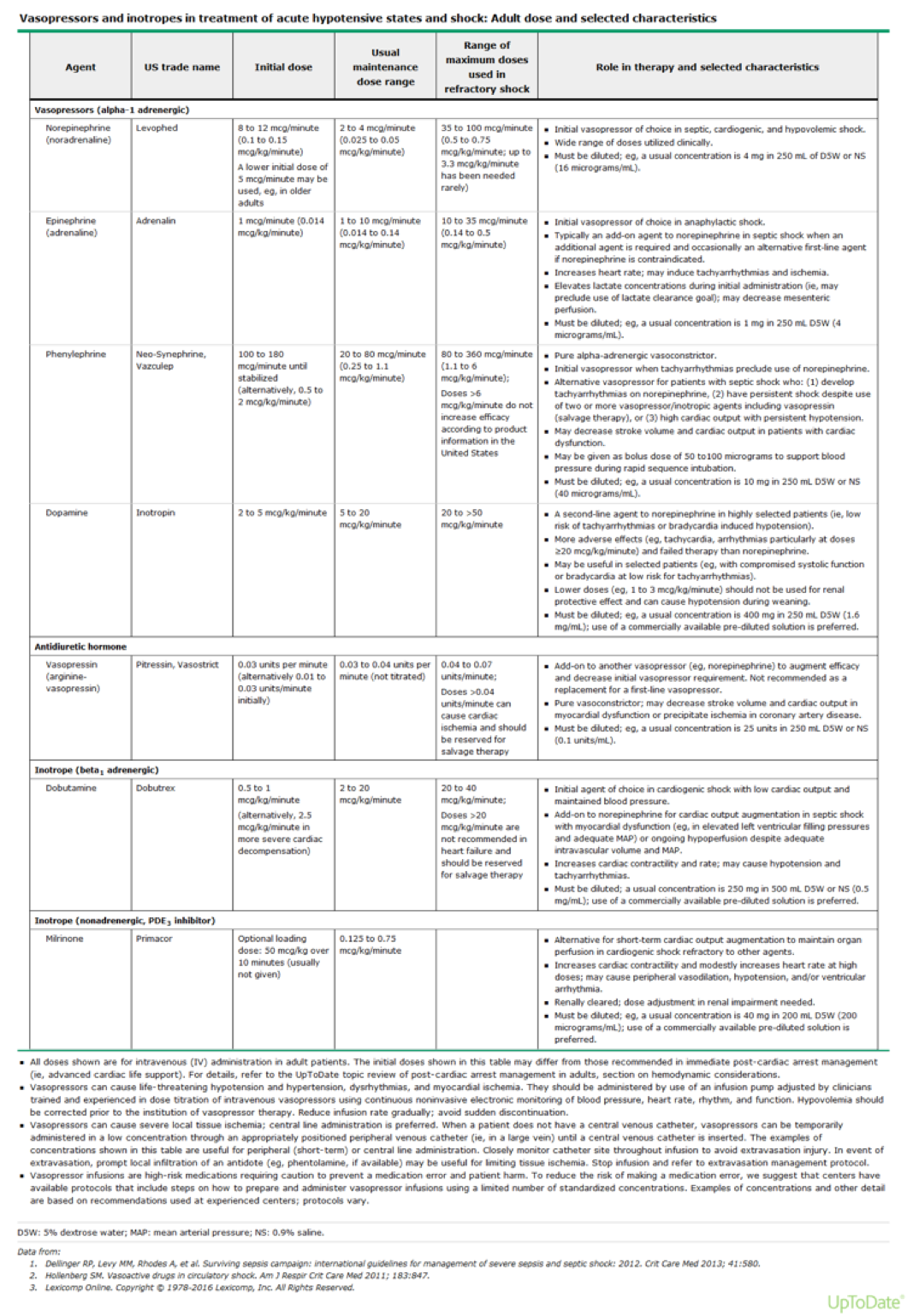
UpToDate



References
You are rounding on a ICU patient who has been on the ventilator for the past 4 days due to respiratory failure from community acquired pneumonia. She has been gradually weaned down to the following settings:
Pressure Support Mode
PEEP – 6 cmH2O
Pressure Support – 8 cmH2O
Oxygen – 0.40
She is A&Ox3 and follows commands. Vital signs show BP – 122/72 mmHg, HR – 78, RR – 15, O2 – 100%, Temp – 99.8.
