
LISTEN TO THE PODCAST HERE
Parathyroid Hormone (PTH)
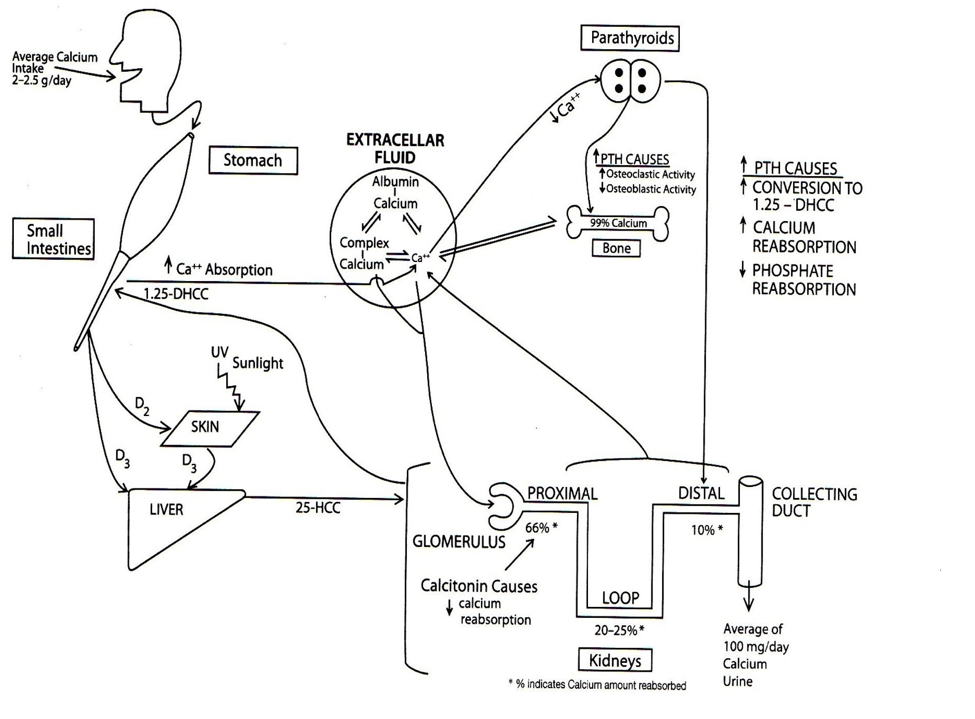
Parathyroid hormone (PTH) is created and stored in the parathyroid glands and is mainly secreted in response to low serum ionized calcium levels.
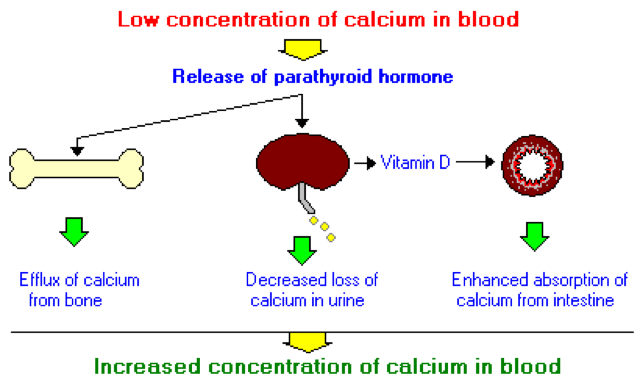
PTH increases serum calcium by 3 main mechanisms:
- Skeletal Actions
- 2 phases
- Mobilize calcium from skeletal stores that are immediately accessible
- Increase osteoclastic activity
- 2 phases
- Renal Actions
- 3 phases
- Increases reabsorption of calcium
- Mainly passively in proximal tubule
- Can also be actively transported in the cortical thick ascending limb of the loop of Henle and distal convoluted tubules
- Inhibits reabsorption of phosphate
- Occurs in the proximal tubule
- Synthesis of calcitriol
- Stimulates synthesis of 1-alpha hydroxylase to convert calcidiol to calcitriol
- Increases reabsorption of calcium
- 3 phases
- Intestinal Actions
- Increases the intestinal absorption of calcium by calcitriol
Causes of Parathyroid Dysfunction
- Hyperparathyroidism
- Primary
- Hyperfunctioning adenomas (94%)
- Primarily parathyroid chief cells
- Glandular hyperplasia (5%)
- Inferior > superior
- Carcinoma (1%)
- Familial hypocalciuric hypercalcemia (FHH)
- Autosomal dominant defect in calcium-sensing receptor
- Secondary
- Chronic renal disease, malabsorption syndromes
- Hyperfunctioning adenomas (94%)
- Primary
- Hypoparathyroidism
- Iatrogenic
- Postsurgical
- Postradiation
- Autoimmune
- Autoimmune polyglandular syndrome
- Calcium-sensor receptor antibodies
- Genetic
- Abnormal development
- Mutations in calcium-sensing receptor
- Iatrogenic
Signs and Symptoms of Parathyroid Dysfunction
- Hyperparathyroidism
- “Stones”
- Nephrolithiasis (up to 20%)
- Renal insufficiency
- “Bones”
- Decreased bone mineral density
- “Abdominal groans”
- Nausea, vomiting, anorexia
- Peptic ulcer disease
- Pancreatitis
- “Porcelain Thrones”
- Polyuria, constipation
- “Psychiatric moans”
- Depression, psychosis, delirium
- “Fatigue overtones”
- Lethargy, fatigue
- “Stones”
- Hypoparathyroidism
- Acute
- Due to hypocalcemia postsurgery
- Perioral numbness, paraesthesias, muscle cramps, tetany, Chvostek’s sign, Trousseau’s sign
-
- Due to hypocalcemia postsurgery
- Chronic
- Basal ganglia calcifications
- Can cause parkinsonism, dystonia, dementia
- Cataracts
- Dental abnormalities (congenital)
- Dental hypoplasia, defective enamel
- Dermal
- Dry, puffy skin
- Coarse, brittle, and sparse hair
- Brittle nails
- Basal ganglia calcifications
- Acute
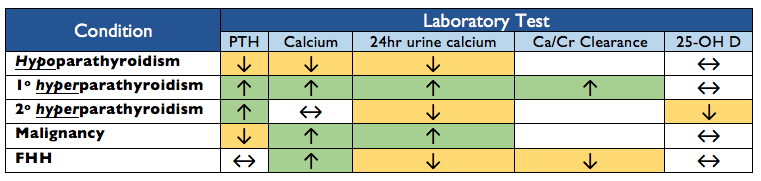
Laboratory Screening
4 main laboratory studies to help differentiate the different causes of parathyroid dysfunction:
- Serum PTH
- Serum calcium
- 24-hour urinary calcium
- Serum 25-hydroxyvitamin D

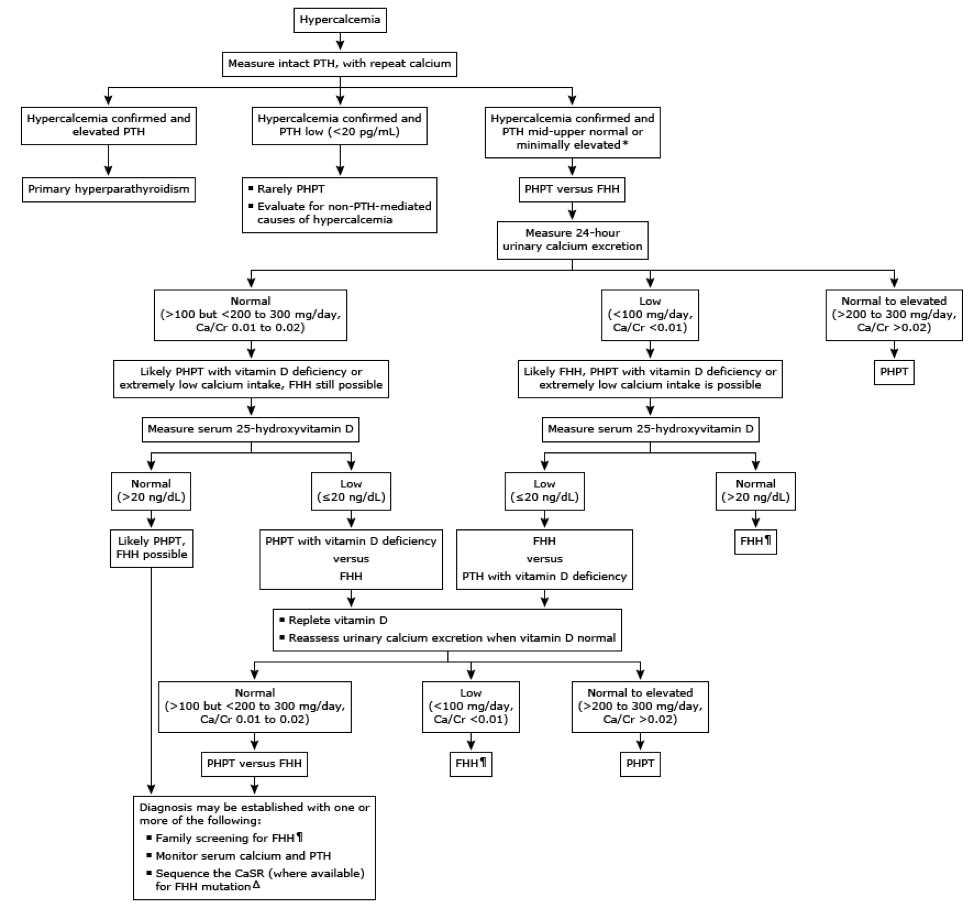
Hypercalcemia Work-up
Management
- Hypoparathyroidism
- Acute (postsurgical)
- 10mL ampule of 10% calcium gluconate in 50mL of D5W over 10-20 minutes followed by a calcium gluconate infusion
- Weaned after calcium ≥ 7.5mg/dL and asymptomatic
- Oral calcitriol (0.5 mcg BID) and calcium carbonate (0.5-2g BID)
- 10mL ampule of 10% calcium gluconate in 50mL of D5W over 10-20 minutes followed by a calcium gluconate infusion
- Chronic
- Oral calcium carbonate or citrate 1000-2000 mg/day
- Oral calcitriol 0.5-2 mcg/day
- Recombinant human PTH can be used to decrease calcium and vitamin D dosing if patients develop side effects
- Acute (postsurgical)
- Hyperparathyroidism
- Primary
- Surgical Indications (any of these with laboratory findings):
- Age < 50
- Serum calcium ≥ 1mg/dL above upper limit of normal
- DXA T-score ≤ -2.5
- Vertebral fracture
- Creatinine clearance < 60 mL/min
- 24-hour urine calcium ≥ 400 mg/day
- Presence of nephrolithiasis
- Preoperative Imaging (Review of parathyroid imaging here)
- Sestamibi-single photon emission computed tomography (MIBI-SPECT)
- Allows for visualization of adenoma, hyperactive glands, or ectopic glands prior to surgery
- Sensitivity – 70-81%, PPV – 91-95%

- Sestamibi-single photon emission computed tomography (MIBI-SPECT)
- Procedure
- Bilateral neck exploration
-
- Medical
- Bisphosphonates
- Inhibits bone resorption and improves bone mass
- Alendronate
- Calcimimetics
- Activate calcium-sensing receptors in the parathyroid gland, which decrease PTH secretion
- Cinacalcet
- Vitamin D
- Bisphosphonates
- Surgical Indications (any of these with laboratory findings):
- Secondary
- Phosphate binders
- Vitamin D supplementation
- Primary

References
- Potts JT, Juppner H. Parathyroid hormone: Molecular biology and regulation. In: Principles of Bone Biology, Bilezikian JP, Raisz LG, Rodan GA (Eds), Academic Press, San Diego 1996. p.325.
- Diaz R, El-Hajj Fuleihan G, Brown EM. Regulation of parathyroid function. In: Handbook of Physiology, Section 7: The Endocrine System, Fray GGS (Ed), Oxford University Press, New York 1999.
- Talmage RV, Mobley HT. Calcium homeostasis: reassessment of the actions of parathyroid hormone. General and Comparative Endocrinology. 2008;156(1):1-8. [pubmed]
- van Abel M, Hoenderop JG, van der Kemp AW, Friedlaender MM, van Leeuwen JP, Bindels RJ. Coordinated control of renal Ca(2+) transport proteins by parathyroid hormone. Kidney International. 2005;68(4):1708-21. [pubmed]
- Bartsch D, Nies C, Hasse C, Willuhn J, Rothmund M. Clinical and surgical aspects of double adenoma in patients with primary hyperparathyroidism. The British Journal of Surgery. 1995;82(7):926-9. [pubmed]
- Ruda JM, Hollenbeak CS, Stack BC. A systematic review of the diagnosis and treatment of primary hyperparathyroidism from 1995 to 2003. Otolaryngology. 2005;132(3):359-72. [pubmed]
- Rafferty MA, Goldstein DP, Rotstein L. Completion thyroidectomy versus total thyroidectomy: is there a difference in complication rates? An analysis of 350 patients. Journal of the American College of Surgeons. 2007;205(4):602-7. [pubmed]
- Silverberg SJ, Bilezikian JP. Evaluation and management of primary hyperparathyroidism. The Journal of Clinical Endocrinology and Metabolism. 1996;81(6):2036-40. [pubmed]
- Coker LH, Rorie K, Cantley L. Primary hyperparathyroidism, cognition, and health-related quality of life. Annals of Surgery. 2005;242(5):642-50. [pubmed]
- Rastogi R, Beauchamp NJ, Ladenson PW. Calcification of the basal ganglia in chronic hypoparathyroidism. The Journal of Clinical Endocrinology and Metabolism. 2003;88(4):1476-7. [pubmed]
- Stein R, Godel V. Hypocalcemic cataract. Journal of Pediatric Ophthalmology and Strabismus. 1980;17(3):159-61. [pubmed]
- Kinirons MJ, Glasgow JF. The chronology of dentinal defects related to medical findings in hypoparathyroidism. Journal of Dentistry. 1985;13(4):346-9.[pubmed]
- Goltzman D, Cole DEC. Hypoparathyroidism. In: Primer on the metabolic bone diseases and disorders of mineral metabolism, 6th ed, Favus MJ. (Ed), American Society of Bone and Mineral Research, Washington, DC 2006. p.216.
- Winer KK, Ko CW, Reynolds JC. Long-term treatment of hypoparathyroidism: a randomized controlled study comparing parathyroid hormone-(1-34) versus calcitriol and calcium. The Journal of Clinical Endocrinology and Metabolism. 2003;88(9):4214-20. [pubmed]
- Bilezikian JP, Brandi ML, Eastell R. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Fourth International Workshop. The Journal of Clinical Endocrinology and Metabolism. 2014;99(10):3561-9. [pubmed]
- Eslamy HK, Ziessman HA. Parathyroid sctinigraphy in patients with primary hyperparathyroidism: 99mTc sestamibi SPECT and SPECT/CT. Radiographics. 2088;28:1461-1476.
