
LISTEN TO THE PODCAST HERE
Epidemiology
Schizophrenia is ranked by the World Health Organization as one of the top mental illnesses in regards to global burden of illness and years lived with disability (YLDs) and disability-adjusted life-years (DALYs).

The estimated prevalence of schizophrenia in the world approaches 1% (that’s 74 million people) and the incidence is around 1.5 per 10,000 population. It is slightly more common in men than women (1.4:1) and they have an overall worse prognosis, but women tend to be diagnosed later in life.

Sham PC
Other Disease Risk
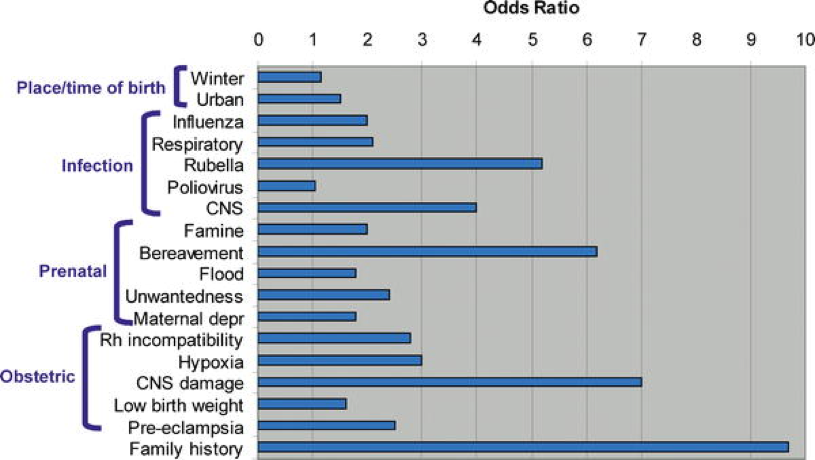
The approach to behavioral medicine conditions is similar to sexually transmitted diseases….in that if you suspect ONE you should screen for ALL. These diseases run in packs and schizophrenia is no exception. There is an increased risk of co-diseases such as depressive disorders, anxiety disorders, substance abuse, and neurologic/endocrinologic disease. There have been many identified risk factors for the development of schizophrenia include environmental, infection, prenatal, obstetric factors, and family history.

Pathogenesis
Unknown at this point, but seems to be a confluence of genetic and environmental factors. Using genome-wide association studies (GWAS), researchers have have found that it is not one or two big genes that cause schizophrenia, but more of a polygenomic effect of multiple small genes with increasingly additive effects. Currently, they have found 500,000 single nucleotide polymorphisms (SNPs) that have been associated with schizophrenia development with 108 of these showing significant association.
Clinical Manifestations
Schizophrenia is a syndrome with impairment in several domains.
- Positive Symptoms
- These are symptoms distort the patient’s reality and/or lead to disorganized thoughts and behaviors
- Called “positive” because they did not have them prior to developing their illness so they were “added” to their psyche
- Hallucinations
- Auditory is most common (40-60%)
- Can included voices, music, machinery
- Visual
- Anything from unformed distortions to fully formed, identifiable objects or human visages
- Somatic
- Sensation of being touched
- Olfactory/Gustatory
- Auditory is most common (40-60%)
- Delusions
- Defined as fixed, false belief even with contradictory evidence
- Up to 80% of patients with schizophrenia
- Can be categorized as:
- Bizarre
- Implausible or impossible
- Non-bizarre
- Understandable, but still untrue
- Content of the delusions can be categorized as delusions of:
- Reference
- Beliefs that seemingly random events are meant for or are in reference to the patient (radio, TV, songs)
- Grandiosity
- Belief the patient has significant importance or power
- Paranoia
- Beliefs that something/someone is trying to affect the patient
- Nihilism
- Beliefs that the patient or other people are dead or don’t exist
- Erotomania
- Beliefs that the patient has a special relationship with someone
- Disorganization
- Reference
- Bizarre
- Schizophrenia is a disorder with disorganized behavior or thoughts. Behaviors can be observed but thoughts can only be inferred from the patient’s speech. Some of these clues are:
- Tangential
- Patient strays from the conversation topic
- Circumstantial
- Patient will answer a question but in a long, roundabout way
- Derailment
- Suddenly switches topics without cue/logic/segue
- Neoligism
- Using made-up words only known to the patient
- Word Salad
- Known words used together in no meaning or pattern
- Tangential
- These are symptoms distort the patient’s reality and/or lead to disorganized thoughts and behaviors
- Negative Symptoms
- Absence of normal processes
- Primary (Deficit Symptoms)
- 2 categories
- Diminished Expression Cluster
- Avolition-Apathy Cluster
- 2 categories
- Secondary
- Any of the above symptoms due to another cause
- Paranoia leading to social isolation
- Unchanging facial expression from antipsychiotic use
- Any of the above symptoms due to another cause

Up To Date. 2016.
- Cognitive Impairment
- Usually precedes positive symptoms and are first observed by family members
- Often one to two standard deviations lower than healthy controls
- Common symptoms include decreases in:
- Processing speed
- Attention
- Working memory
- Verbal/visual learning
- Reasoning
- Executive function
- Comprehension
- Social cognition
- Mood and Anxiety Symptoms
- Higher incidence in patients with schizophrenia than the general population
Physical Manifestations
There are a few physical exam findings that can be seen in patients with schizophrenia that can precipitate further screening.
- Neurologic Disturbances
- Subtle impairments of sensory integration, motor coordination, and sequencing and need to distinguished from normal pathology of the disease and the side effects of medications
- Disease specific
- Right/left confusion
- Agraphesthesia
- Astereognosis
- Catatonia
- Medication Induced
- Extrapyramidal
- Tremor, bradykinesia, dystonia, tardive dyskinesia
- Metabolic Disturbances
- Weight gain, diabetes development, cardiovascular disease
- Extrapyramidal
Disease Course
The presentation and disease is highly variable and differ in regards to onset (rapid vs slow), symptom presentation (continuous vs intermittent) and outcome (poor vs controlled). Each patient with the suspicion of schizophrenia should be screened for these variables.
DSM-V Criteria for Diagnosis
- 2 or more characteristic symptoms (one must be delusions, hallucinations, or disorganized speech) present for a significant portion of time during a one-month period:
- Delusions
- Hallucinations
- Disorganized speech
- Grossly disorganized or catatonic behavior
- Negative symptoms
- For a significant portion of the time since the onset of the disturbance, one or more major areas of functioning such as work, interpersonal relations, or self-care are markedly below the level achieved prior to the onset.
- When the onset is in childhood or adolescence:
- Failure to achieve expected level of interpersonal, academic, or occupational achievement.
- When the onset is in childhood or adolescence:
- Continuous signs of the disturbance persist for at least six months.
- The six-month period must include at least one month of symptoms (or less if successfully treated and may include periods of prodromal or residual symptoms.
- Schizoaffective disorder and mood disorder with psychotic features have been ruled out because either:
- (1) no major depressive, manic, or mixed episodes have occurred concurrently with the active-phase symptoms; or
- (2) if mood episodes have occurred during active-phase symptoms, their total duration has been brief relative to the duration of the active and residual periods.
- The disturbance is not due to the direct physiological effects of a substance (eg, a drug of abuse or medication) or a general medical condition.
- If the patient has a history of autistic disorder or another pervasive developmental disorder, the additional diagnosis of schizophrenia is made only if prominent delusions or hallucinations are also present for at least a month (or less if successfully treated)
Differential Diagnosis
There are several other conditions that can mimic schizophrenia and need to be assessed during screening or diagnosis.
- Schizophreniform
- Meets all criteria for schizophrenia, but has had < 6 months of symptoms
- Schizoaffective, bipolar, and major depressive disorders
- More mood components than disorganized thoughts or behaviors
- Substance abuse or withdrawal
- Schizotypal disorders
- Odd behaviors or beliefs but not to the level of delusions or hallucinations
- Schizoid personality disorder
- Long standing pattern of little interest in social relationships
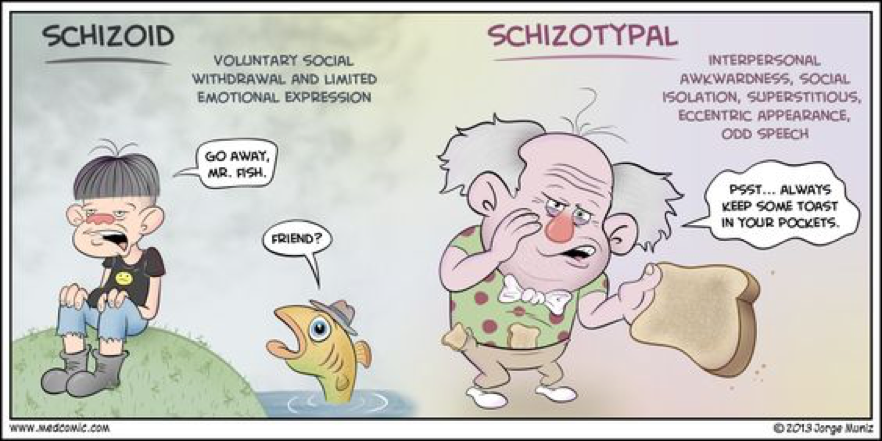
MedComic
Schizophrenia Diagnostic Algorithm

Up To Date. 2016.
Management
Two categories of treatments in schizophrenia:
- Acute Phase
- Psychotic relapse in a patient with a known diagnosis, or the first episode of psychosis in an undiagnosed patient.
- Goal of acute management to decrease agitation and increase therapeutic medication
- Maintenance Phase
- Recovered from acute psychotic event
- Goal of maintenance is minimize symptoms and functional impairments, avoid relapses, and promote recovery
Prescreening Considerations
- BMI, waist circumference, heart rate, blood pressure
- Signs of movement disorder
- Extrapyramidal symptoms
- Akathisia, parkinsonism, dystonias
- Tardive dyskinesia
- Extrapyramidal symptoms
- Laboratory Studies (when feasible)
- CBC, BMP, lipid profile, LFT, TFT
- EKG
Antipsychotic Medications
- 1st generation (Typical)
- All antipsychotics marketed before 1989 (when clozapine came out)
- 2nd generation (Atypical)
- Everything after clozapine
- Cause fewer extrapyramidal side effects
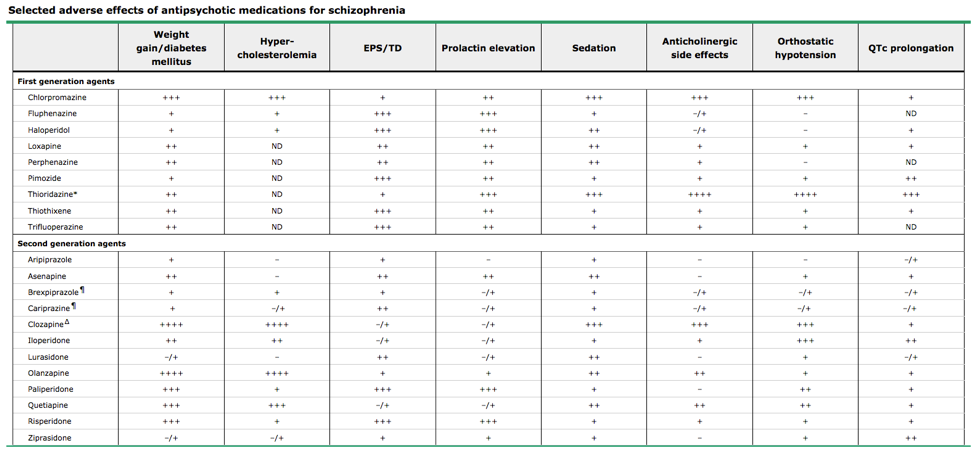
Up To Date. 2016.
Treatment Considerations
There are several medications available as IM, extended release injections that can be helpful in chronic maintenance in non-adherent patients.
Cottage Physician on Hysteria
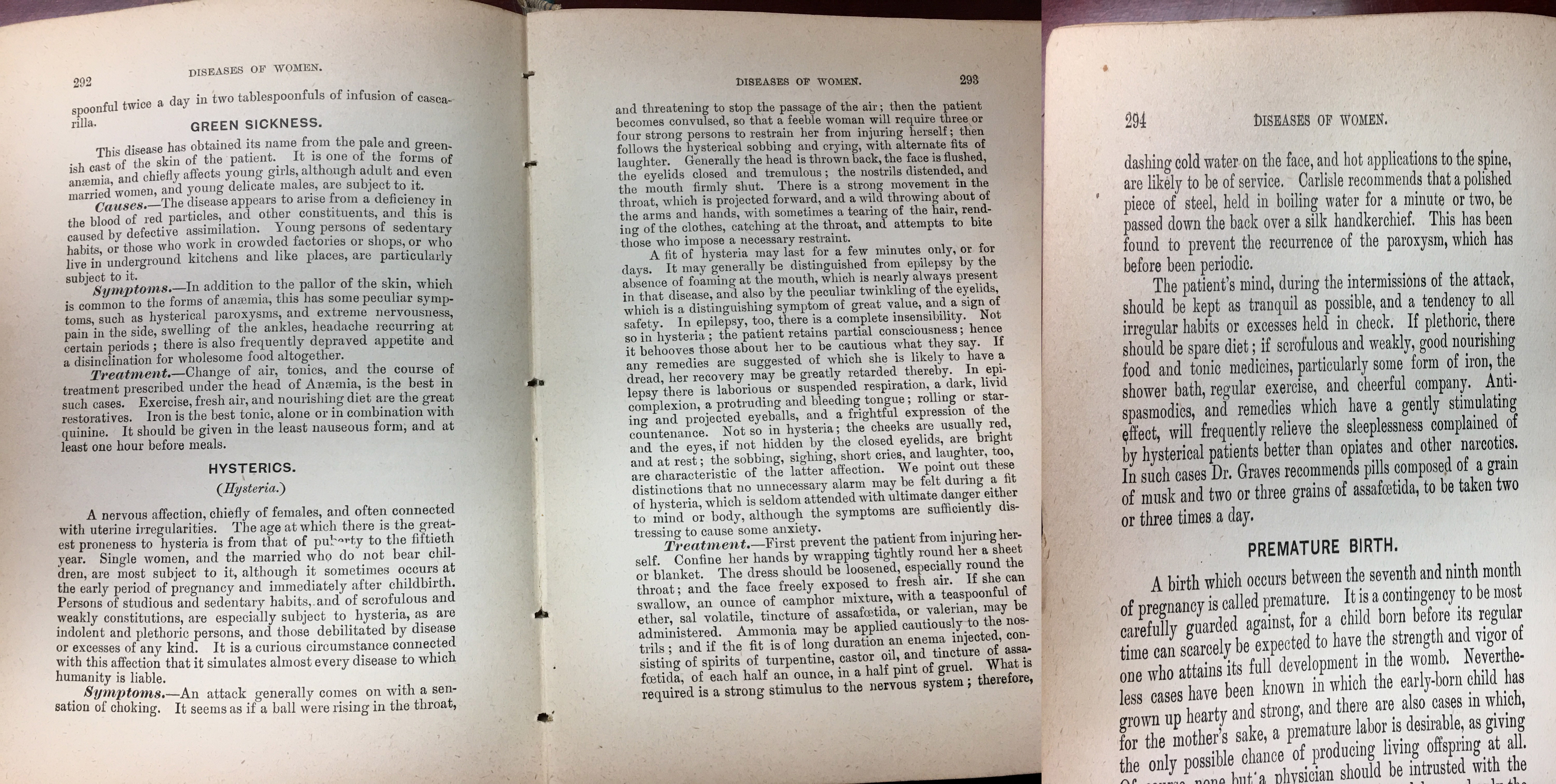
Cottage Physician, 1893.
References
- Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. 2016;3(2):171-8. [pubmed]
- McGrath J, Saha S, Chant D, Welham J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiologic Reviews. 2008;30:67-76. [pubmed]
- Abel KM, Drake R, Goldstein JM. Sex differences in schizophrenia. International Review of Psychiatry. 2010;22(5):417-28. [pubmed]
- Sham PC, MacLean CJ, Kendler KS. A typological model of schizophrenia based on age at onset, sex and familial morbidity. Acta Psychiatrica Scandinavica. 1994;89(2):135-41. [pubmed]
- Grossman LS, Harrow M, Rosen C, Faull R, Strauss GP. Sex differences in schizophrenia and other psychotic disorders: a 20-year longitudinal study of psychosis and recovery. Comprehensive Psychiatry. 2008;49(6):523-9. [pubmed]
- Usall J, Ochoa S, Araya S, Márquez M, . Gender differences and outcome in schizophrenia: a 2-year follow-up study in a large community sample. Journal of the Association of European Psychiatrists. 2003;18(6):282-4. [pubmed]
- Schizophrenia Working Group of the Psychiatric Genomics Consortium. Biological insights from 108 schizophrenia-associated genetic loci. Nature. 2014;511(7510):421-7. [pubmed]
- Owen MJ, Sawa A, Mortensen PB. Schizophrenia. Lancet. 2016;388(10039):86-97. [pubmed]
- Thomas P, Mathur P, Gottesman II, Nagpal R, Nimgaonkar VL, Deshpande SN. Correlates of hallucinations in schizophrenia: A cross-cultural evaluation. Schizophrenia Research. 2007;92(1-3):41-9. [pubmed]
- Andreasen NC, Olsen S. Negative v positive schizophrenia. Definition and validation. Archives of General Psychiatry. 1982;39(7):789-94. [pubmed]
- Nuechterlein KH, Barch DM, Gold JM, Goldberg TE, Green MF, Heaton RK. Identification of separable cognitive factors in schizophrenia. Schizophrenia Research. 2004;72(1):29-39. [pubmed]
- Gold JM, Hahn B, Strauss GP, Waltz JA. Turning it upside down: areas of preserved cognitive function in schizophrenia. Neuropsychology Review. 2009;19(3):294-311. [pubmed]
- Heinrichs DW, Buchanan RW. Significance and meaning of neurological signs in schizophrenia. The American Journal of Psychiatry. 1988;145(1):11-8. [pubmed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), American Psychiatric Association, Arlington, VA 2013.
- Buchanan RW, Kreyenbuhl J, Kelly DL. The 2009 schizophrenia PORT psychopharmacological treatment recommendations and summary statements. Schizophrenia Bulletin. 2010;36(1):71-93. [pubmed]

Pingback: Alcohol Abuse Graphs | SaappadU