*** LISTEN TO THE PODCAST HERE ***




Question
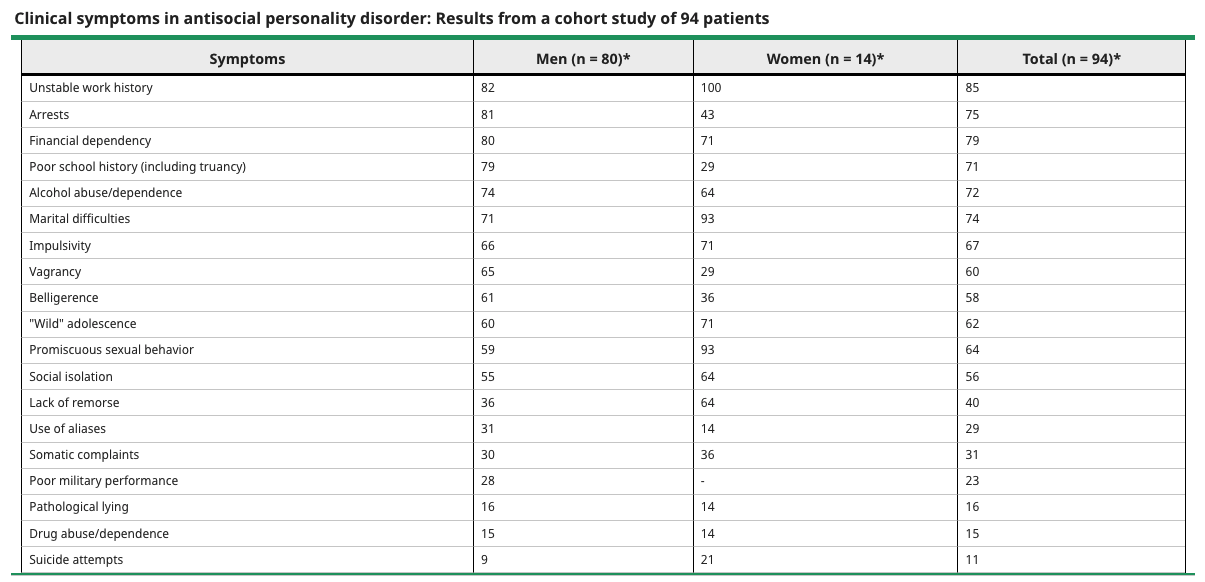
You are asked to evaluate a 23yo male prisoner for underlying psychiatric illness prior to standing trial for his third aggravated assault arrest in 12 months. During your discussion, he discloses that he doesn’t hold jobs down very well because “his bosses are idiots”, does not speak with his family, and prefers to not have friends because “everybody is stupid”. He was expelled from 3 different high schools and finally dropped out at 16. In reviewing his criminal record with his attorney, it is revealed he has been arrested 9 times starting at age 14 for theft, burglary, assault, and intoxication infractions.
Answer

Korsakoff Syndrome
Other Known Aliases – none
Definition – chronic, irreversible amnestic disorder caused by thiamine deficiency classically associated with longstanding alcohol use
Clinical Significance – there are seven major symptoms of Korsakoff syndrome that can be seen clinically:
This is classically taught as a continuation of Wernicke’s encephalopathy, though patients may not present in early stages.

History – Named after Sergei Sergeievich Korsakoff (1854-1900), who was a Russian neuropsychiatrist and received his medical doctorate from Moscow State University in 1875. He would go on to gain fame in fields of neurology and psychiatry culminating in his appointment as professor extraordinarius at a dedicated psychiatric hospital in Moscow and helping to found the Moscow Society of Neuropathologists and Psychiatrists. His eponymous condition was first described in 1887 in his graduate thesis entitled “Alcoholic Paralysis”
References

Question
You are asked to evaluate a 23yo male prisoner for underlying psychiatric illness prior to standing trial for his third aggravated assault arrest in 12 months. During your discussion, he discloses that he doesn’t hold jobs down very well because “his bosses are idiots”, does not speak with his family, and prefers to not have friends because “everybody is stupid”. He was expelled from 3 different high schools and finally dropped out at 16. In reviewing his criminal record with his attorney, it is revealed he has been arrested 9 times starting at age 14 for theft, burglary, assault, and intoxication infractions.
Tourette Syndrome
Other Known Aliases – Brissaud’s Disease
Definition – neurodevelopmental disorder characterized by motor and vocal tic with onset during childhood
Clinical Significance – the exact cause is still largely unknown, but likely results from a disturbance in the cortico-striatal-thalamic-cortical (mesolimbic) circuit, which leads to disinhibition of the motor and limbic system. There are no specific tests to confirm and is a clinical diagnosis. The severity of the tics largely decreases, and in some instances disappears, in adolescence and adulthood.
History – Named after Georges Gilles de la Tourette (1857-1904), a French neurologist who recieved his medical doctorate from University of Poitiers at the age of 16. He subsequently moved to Paris to train at the famous Laennec Hospital and Salpêtrière Hospital under Jean Martin Charcot. Under the tutelage of Charcot, he made tremendous strides in the area of psychotherapy, hysteria, psychology, and neurology and described his eponymous condition in a nine patient case series in 1884. In a rather cruel twist of fate, he was shot in the neck by a patient he had treated with hypnotism in 1893, fell into a deep depression, committed to a psychiatric hospital due to tertiary neurosyphilis, and died there in 1904.

References
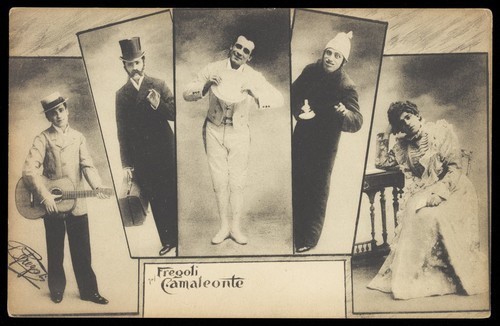
Frégoli Delusion
Other Known Aliases – delusion of doubles
Definition – mistaken belief that some person currently present in the deluded person’s environment (typically a stranger) is a familiar person in disguise.
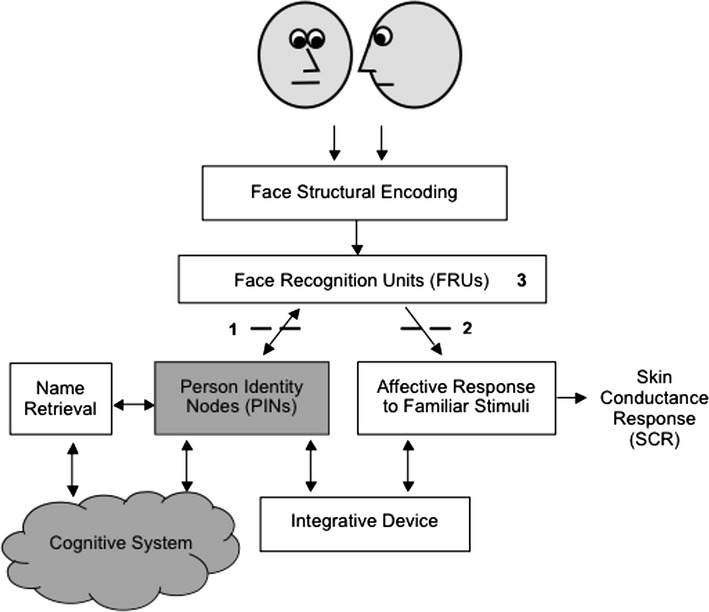
Clinical Significance – to the patient, the stranger is believed to be psychologically identical to this known person (who is not present) even though the deluded person perceives the physical appearance of the stranger as being different from the known person’s typical appearance. There are 4 subtypes:

History – this syndrome was first published in 1927 by Courbon and Fail who describe a case of a young woman who believed she was being pursued by two Parisian actresses in disguise. They named this delusional syndrome after Leopoldo Frégoli, who was an Italian stage actor with an extraordinary ability to impersonate and mimic others on stage.



References

Link to SAMHSA-HRSA Page for Screening Tools




CAGE-AID

Alcohol Use Disorder Identification Test (AUDIT)

Drug Abuse Screening Test (DAST-10)

Humiliation, Afraid, Rape, Kick (HARK)
Hurt, Insult, Threaten, Scream (HITS) Scale

Woman Abuse Screening Tool (WAST)

Question
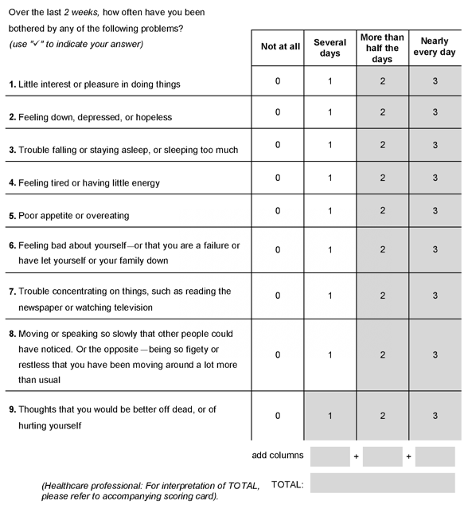
A 20yo man, with no significant past medical history, is brought in by his parents for evaluation of concerning behaviors. They state he often feels he “needs” to arrange the items in his room in a certain way and becomes very agitated if they are moved. He also must make sure that there is no dirt on his shoes before he walks in his room and is meticulous in his cleaning endeavors every day. His parents are worried about his level of functioning and ability to move out and maintain his own apartment. He denies any thoughts of self-harm, homicidal ideations, or audio-visual hallucinations. On physical examination, he seems composed, non-distracted, and answers all questions appropriately. When asked about these behaviors, he recognizes that they are a problem, but states he can’t relax and has severe anxiety unless these are taken care of.
Answer
The most likely diagnosis is obsessive compulsive disorder and is defined by the DSM-V using the below criteria:
A. Presence of obsessions, compulsions, or both
B. The obsessions or compulsions are time-consuming (eg, take more than one hour per day) or cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
C. The obsessive-compulsive symptoms are not attributable to the physiological effects of a substance (eg, a drug of abuse, a medication) or another medical condition.
D. The disturbance is not better explained by the symptoms of another mental disorder.
DSM-V Specifiers
Charles Bonnet Syndrome
Other Known Aliases – visual release hallucinations
Definition – symptoms of visual hallucinations that occur in patients with visual loss

Clinical Significance – these release hallucinations can be simple, non-formed images (such as lines, flashes, shapes, etc.) or the can be formed images (such as people, animals, scenes, etc.). These patients can often be missed diagnosed as psychosis or early dementia. Diagnosis is made in the absence of other psychiatric illness or other causes of hallucinations.
History – Named after Charles Bonnet (1720-1793), who was a Genevan naturalist who was a lawyer by trade, but fascinated by the natural sciences. He spent the majority of career observing and studying insects, germ theory, and philosophy. He described the eponym that bears his name in 1760 in his book “Essai analytique sur les facultés de l’âme“, where he described the hallucinations of his 87yo grandfather who was nearly blind from cataracts


References

