

57-year-old male, with controlled hypertension, presents to emergency department with a 2-hour history of a central, dull, chest pain that does not radiate. He rates it as a 4/10 in severity and denies any aggravating or alleviating factors. He reports some mild nausea and what he reports as “reflux” during this event as well. He denies shortness of breath, vomiting, arm radiation, back radiation, abdominal pain, dizziness, or syncope. His father has HTN, HLP, and had a non-fatal AMI at 62-years-old. He is a never smoker. His BMI is 27.3.
Vital signs show BP-122/82, HR-93, RR-16, O2-100% on room air, and temp-98.0.
Physical exam reveals:
HEENT – NC/AT
Skin – no diaphoresis
Cardiovascular – RRR without M/G/R
Pulmonary – CTA without adventitial breath sounds
Abdomen – S/ND, mild epigastric tenderness to deep palpation
Peripheral Vascular – 2+ pulses throughout
Neuro – A&Ox3, 5/5 strength throughout
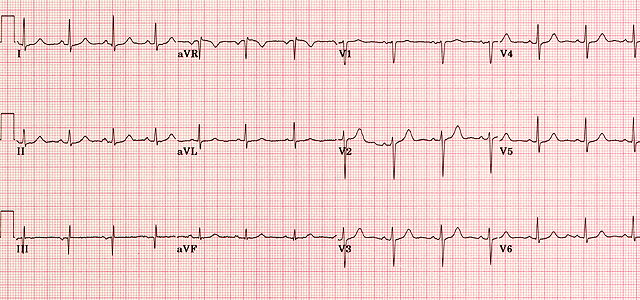
EKG is below:
Laboratory Screening:
High-sensitivity troponin (hs-cTnI) – 0.02 ng/dL
CK-MB – 39 U/L
Total CK – 264 U/L
Myoglobin – 22 ng/mL
