*** LISTEN TO THE PODCAST HERE ***



***LISTEN TO THE PODCAST HERE***





***LISTEN TO THE PODCAST HERE***
Anterior
Posterior



***LISTEN TO THE PODCAST HERE***


Question
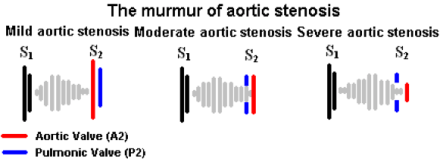
73yo man, with a history of hypertension and coronary disease, is brought into the emergency room after a witnessed syncopal episode at home. He reported some mild exertional chest pain over the past few days, but states that it improved with rest. Vital signs are BP-180/98, HR-74, RR-12, and O2-100%. He is currently in no distress and not diaphoretic. Physical examination revealed a systolic murmur over the 2nd right intercostal space. A CT was ordered to rule-out PTE in the setting of chest pain and syncope and is below, along with the murmur.
Answer


Question
73yo man, with a history of hypertension and coronary disease, is brought into the emergency room after a witnessed syncopal episode at home. He reported some mild exertional chest pain over the past few days, but states that it improved with rest. Vital signs are BP-180/98, HR-74, RR-12, and O2-100%. He is currently in no distress and not diaphoretic. Physical examination revealed a systolic murmur over the 2nd right intercostal space. A CT was ordered to rule-out PTE in the setting of chest pain and syncope and is below, along with the murmur.
Question
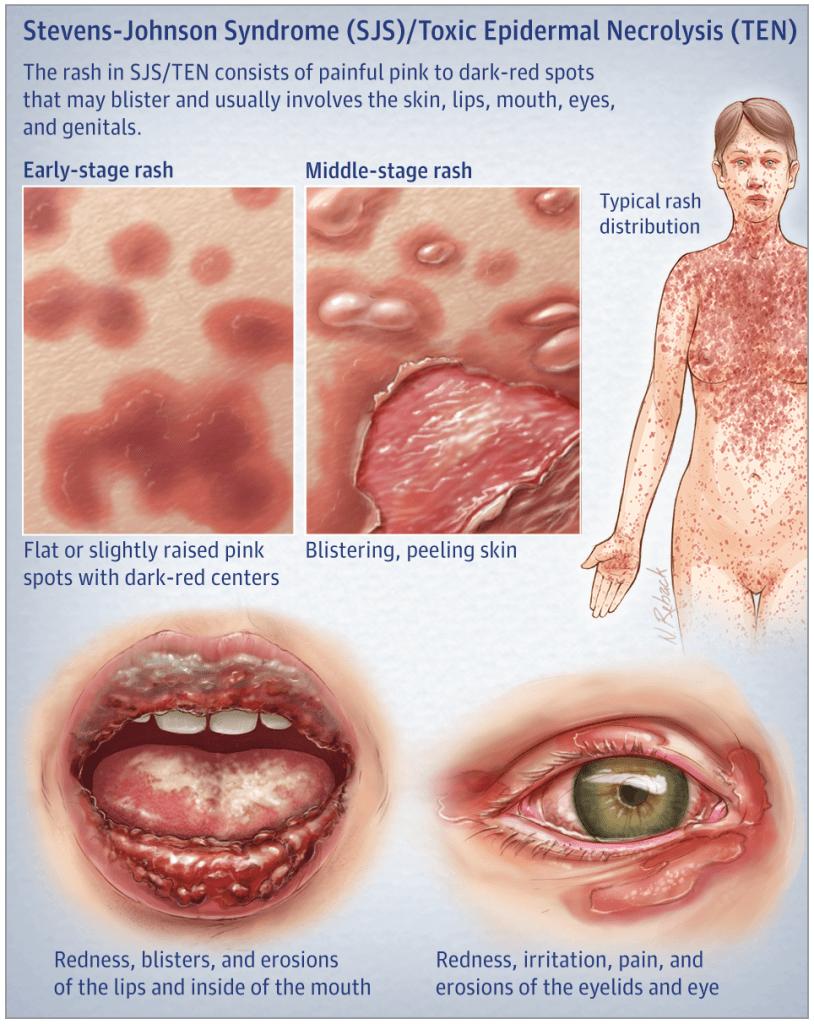
A 29yo patient is seen for a severe drug reaction after starting lamotrigine (Lamictal) for new-onset epilepsy. She has significant desquamation of her mucous membranes as well as large patches of denuded epidermis with multiple bullae present.

Answer
The main clinical difference between SJS and TEN is the severity and degree of involvement. SJS classically is < 10% TBSA involvement, where as TEN is > 30% TBSA.

Question
A 29yo patient is seen for a severe drug reaction after starting lamotrigine (Lamictal) for new-onset epilepsy. She has significant desquamation of her mucous membranes as well as large patches of denuded epidermis with multiple bullae present.

Le Fort Fractures
Other Known Aliases – transfacial fracture of the midface
Definition – These fractures involve the maxillary bone and are graded based on their direction and involvement of surrounding structures. The key distinguishing feature of this type of fracture is separation of the pterygoid plates from the maxillary sinuses.
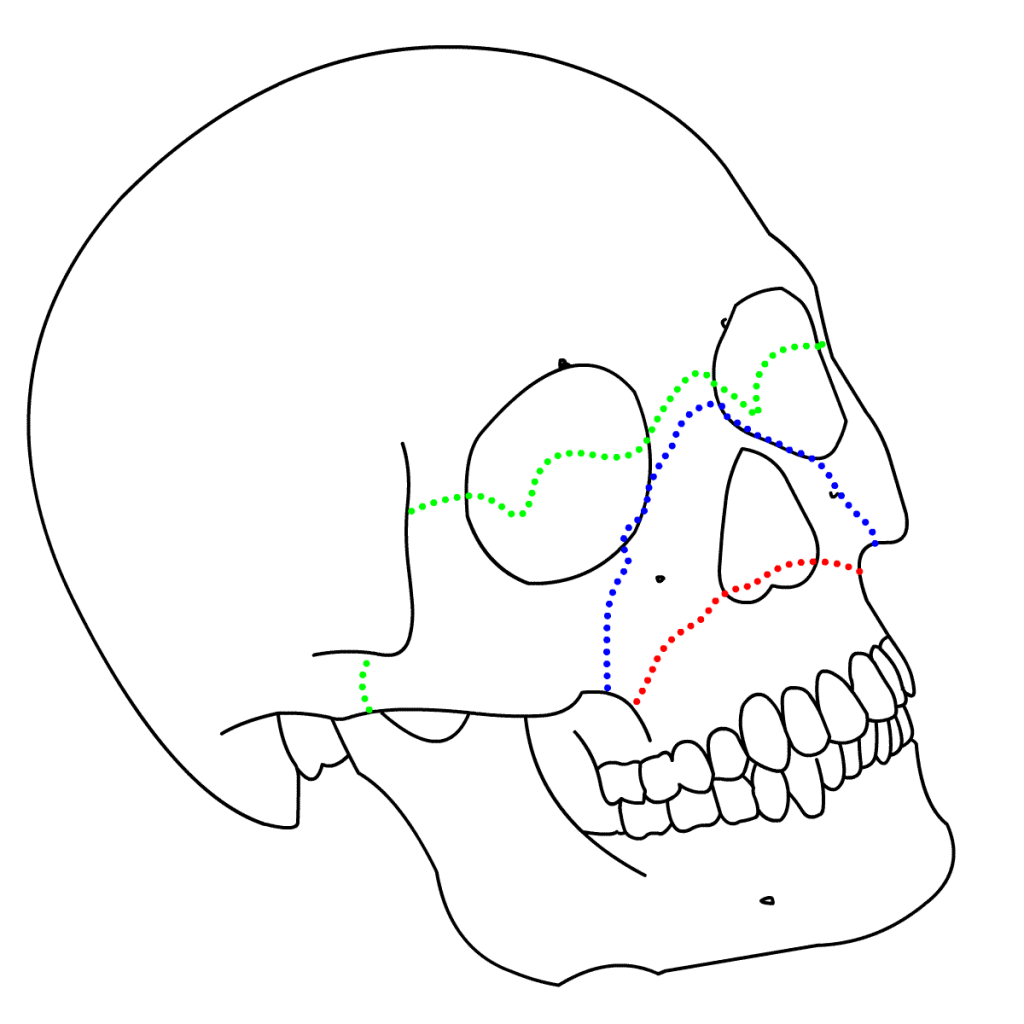
Clinical Significance – Continuity of the pterygoid plates is essential for midface structural stability and any disruption requires surgical fixation. There are three types of Le Fort fractures:

History – Named after René Le Fort (1869-1951), who was a French surgeon and received his medical doctorate at the age of 21 while serving in the French military. He taught and practice in Lille, France for the majority of his career. He served his country numerous times when called to serve as a military physician, as well as coming out of retirement during World War II to teach at the University of Lille to replace colleagues called to the war effort. He published the findings of his eponymous conditions in 1901 in a treatise entitled “Étude expérimentale sur les fractures de la mâchoire supérieure”, where he described his experiments of dropping cannon balls from varying directions and heights on the faces of cadavers to describe the predictable injury patterns
References
Question
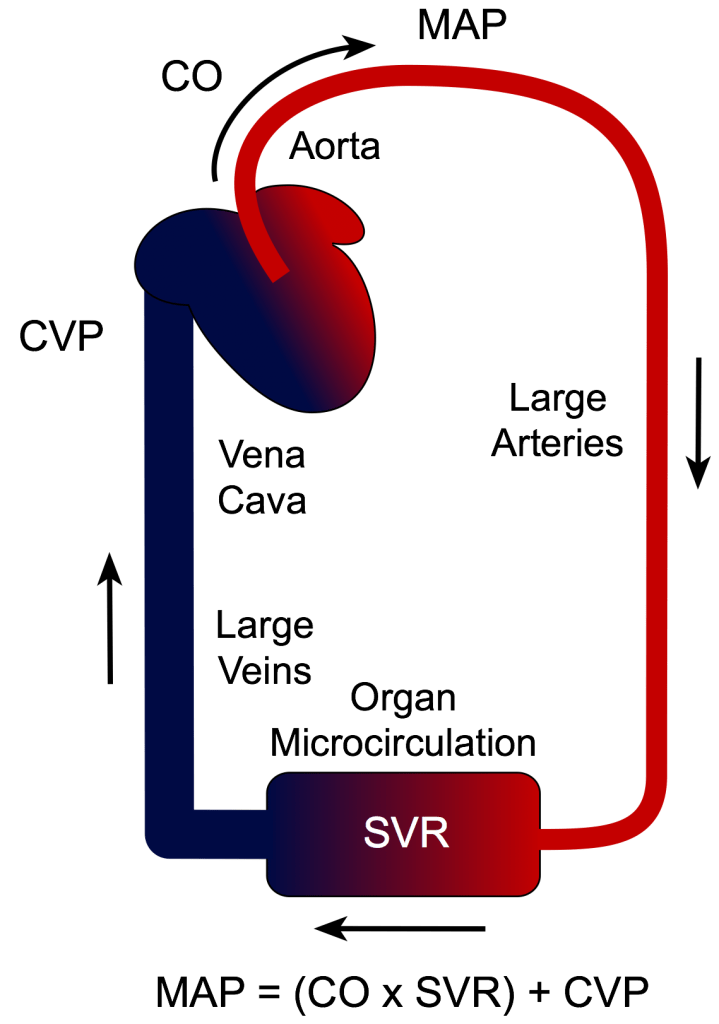
A large part of critical care and ICU management revolves around hemodynamic monitoring and support. But…..we typically don’t use traditional blood pressure (systolic and diastolic) numbers directly.
We use MAP!!!
Answer


References
