
***LISTEN TO THE PODCAST HERE***
Definition
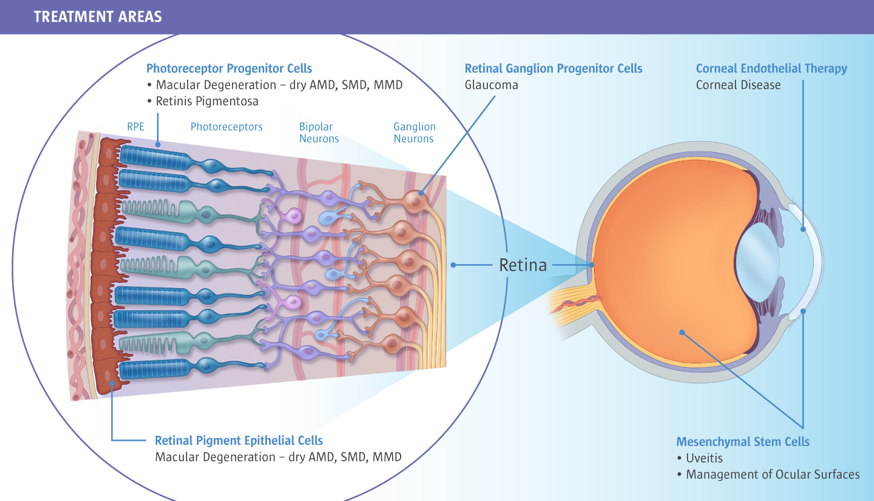
A retinal detachment is defined as a separation of the multilayer neurosensory retina from the underlying retinal pigment epithelium and choroid.
Epidemiology
Retinal detachments have been reported to occur in 6-20 per 100,000 population worldwide, but there is wide variability in incidence between the types. Risk factors include:
- Myopia (most common)
- Age (50-75yr)
- Previous eye surgery or injury
- Use of fluoroquinolones
- History of glaucoma
- Family history of retinal detachment
- Diabetes
- Hypertension
Pathophysiology and Types
There are 2 main types of retinal types and the pathophysiology is slightly different.
- Rhegmatogenous (most common)
- Full-thickness tear caused by vitreous traction on the retina
- Not to be confused with tractional detachment
- RRD à tear 1st, then vitreous traction forces fluid in
- TRD à traction pulls the layers away, but no tear
- Most common site is a posterior vitreous detachment
- Typically take weeks to months to fully develop
- Traumatic retinal detachment can occur from surgery or injury
- Not to be confused with tractional detachment
- Full-thickness tear caused by vitreous traction on the retina
- Nonrhegmatogenous
- Tractional
- Vitreous traction separates the layers and neovascularization from DM, HTN, sickle cell causes fluid to accumulate
- Exudative
- Fluid accumulation from inflammatory states or ocular malignancies causes the separation of layers
- Tractional

Signs and Symptoms
- Mostly slow onset (weeks to months), but can be acute if traumatic
- Increase, or worsening of floaters
- Multiple, cob-web like
- Single, large
- Romans called this “mosca volante” –> large housefly
- Gradual loss of peripheral vision (“curtain pulled over eye”)
- Decrease in visual acuity once the macula is involved
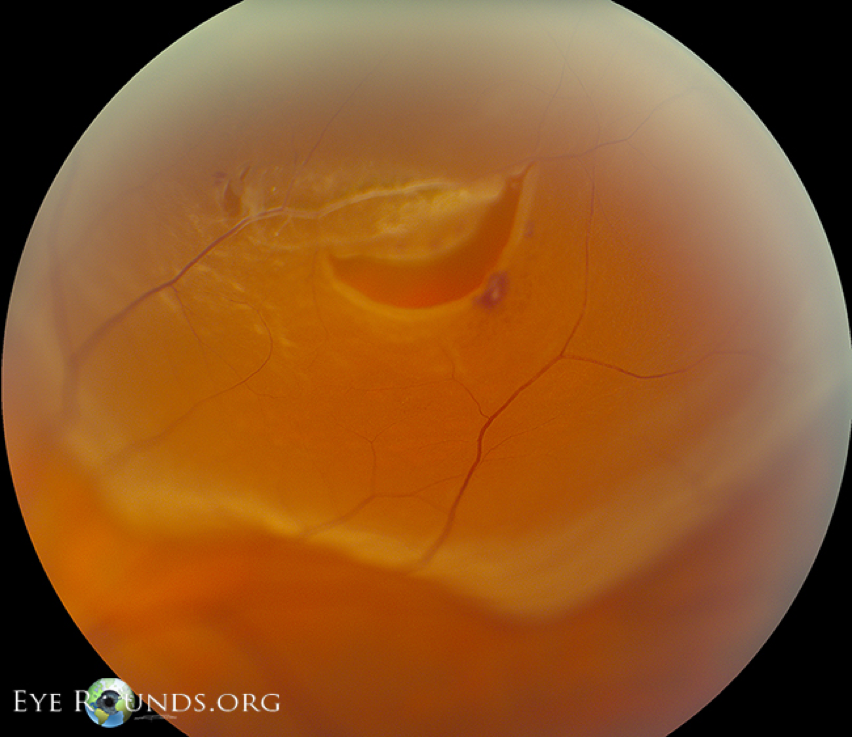
Physical Exam
All patients with any eye complaint should have visual acuity checked and documented. If you suspect a detachment from the history, visual fields should be assessed. Fundoscopic exam should be performed to look for any gross retinal defects. All patients with a suspected retinal detachment should be referred for urgent evaluation by an ophthalmologist for dilated retinal exam with slitlamp. The test of choice is a 360o scleral depressed examination using an indirect ophthalmoscope.
Rhegmatogenous Retinal Detachment

Tractional Retinal Detachment

Exudative Retinal Detachment
Imaging
Ultrasound technology is getting better and better and ocular scanning can see detachments at the bedside in the hands of a competent provider.
Treatment
- Detachment without tear
- Reassurance that floaters with resolve over 3-12 months
- Tear without detachment
- Risk of detachment is around 30% if left untreated
- 2 options
- Laser Retinopexy
-

- Cryoretinopexy
- (see below scleral buckling video)
- Both take approximately 2 weeks to form strong adhesions
- Tear with detachment
- Without treatment, will progress to complete vision loss
- Small tears
- Laser or cryoretinoplexy
- Large tears
- Pneumatic retinopexy (office)
- Cryoretinopexy with injection of gas bubble and head position to tamponade the tear
- 24-48hr for fluid reabsorption and retinal re-attachment
- 70-80% 1st time success
-
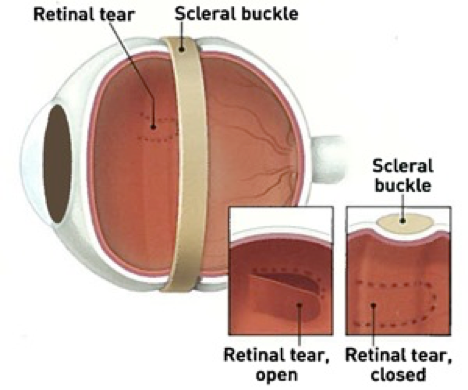
- Scleral buckle (OR)
- Cryoretinopexy with suturing of an exoplant to the outside of the sclera, which causes an indentation in the wall of the eye

-
- 80-90% 1st time success
- Vitrectomy
- Removal of central and peripheral vitreous humor with gas or liquid injection
- 80-90% 1st time success
-
- Pneumatic retinopexy (office)

References
- Mitry D, Charteris DG, Fleck BW, Campbell H, Singh J. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. The British Journal of Ophthalmology. 2010;94(6):678-84. [pubmed]
- Wilkes SR, Beard CM, Kurland LT, Robertson DM, O’Fallon WM. The incidence of retinal detachment in Rochester, Minnesota, 1970-1978. American Journal of Ophthalmology. 1982;94(5):670-3. [pubmed]
- Haimann MH, Burton TC, Brown CK. Epidemiology of retinal detachment. Archives of Ophthalmology (Chicago, Ill. : 1960). 1982; 100(2):289-92. [pubmed]
- Risk factors for idiopathic rhegmatogenous retinal detachment. The Eye Disease Case-Control Study Group. American Journal of Epidemiology. 1993;137(7):749-57. [pubmed]
- Pasternak B, Svanström H, Melbye M, Hviid A. Association between oral fluoroquinolone use and retinal detachment. JAMA. 2013;310(20):2184-90. [pubmed]
- Go SL, Hoyng CB, Klaver CC. Genetic risk of rhegmatogenous retinal detachment: a familial aggregation study. Archives of Ophthalmology (Chicago, Ill. : 1960). 2005;123(9):1237-41. [pubmed]
- Hikichi T, Trempe CL, Schepens CL. Posterior vitreous detachment as a risk factor for retinal detachment. Ophthalmology. 1995;102(4):527-8. [pubmed]
- Wolfensberger TJ, Tufail A. Systemic disorders associated with detachment of the neurosensory retina and retinal pigment epithelium. Current Opinion in Ophthalmology. 2000;11(6):455-61. [pubmed]
- Hollands H, Johnson D, Brox AC, Almeida D, Simel DL, Sharma S. Acute-onset floaters and flashes: is this patient at risk for retinal detachment? JAMA. 2009;302(20):2243-9. [pubmed]
- Byer NE. Natural history of posterior vitreous detachment with early management as the premier line of defense against retinal detachment. Ophthalmology. 1994;101(9):1503-13. [pubmed]
- Coffee RE, Westfall AC, Davis GH, Mieler WF, Holz ER. Symptomatic posterior vitreous detachment and the incidence of delayed retinal breaks: case series and meta-analysis. American Journal of Ophthalmology. 2007;144(3):409-413. [pubmed]
- D’Amico DJ. Clinical practice. Primary retinal detachment. The New England Journal of Medicine. 2008;359(22):2346-54. [pubmed]
- Hilton GF, Tornambe PE. Pneumatic retinopexy. An analysis of intraoperative and postoperative complications. The Retinal Detachment Study Group. Retina (Philadelphia, Pa.). 1991;11(3):285-94. [pubmed]
- Tornambe PE, Hilton GF. Pneumatic retinopexy. A multicenter randomized controlled clinical trial comparing pneumatic retinopexy with scleral buckling. The Retinal Detachment Study Group. Ophthalmology. 1989;96(6):772-83. [pubmed]
