Question
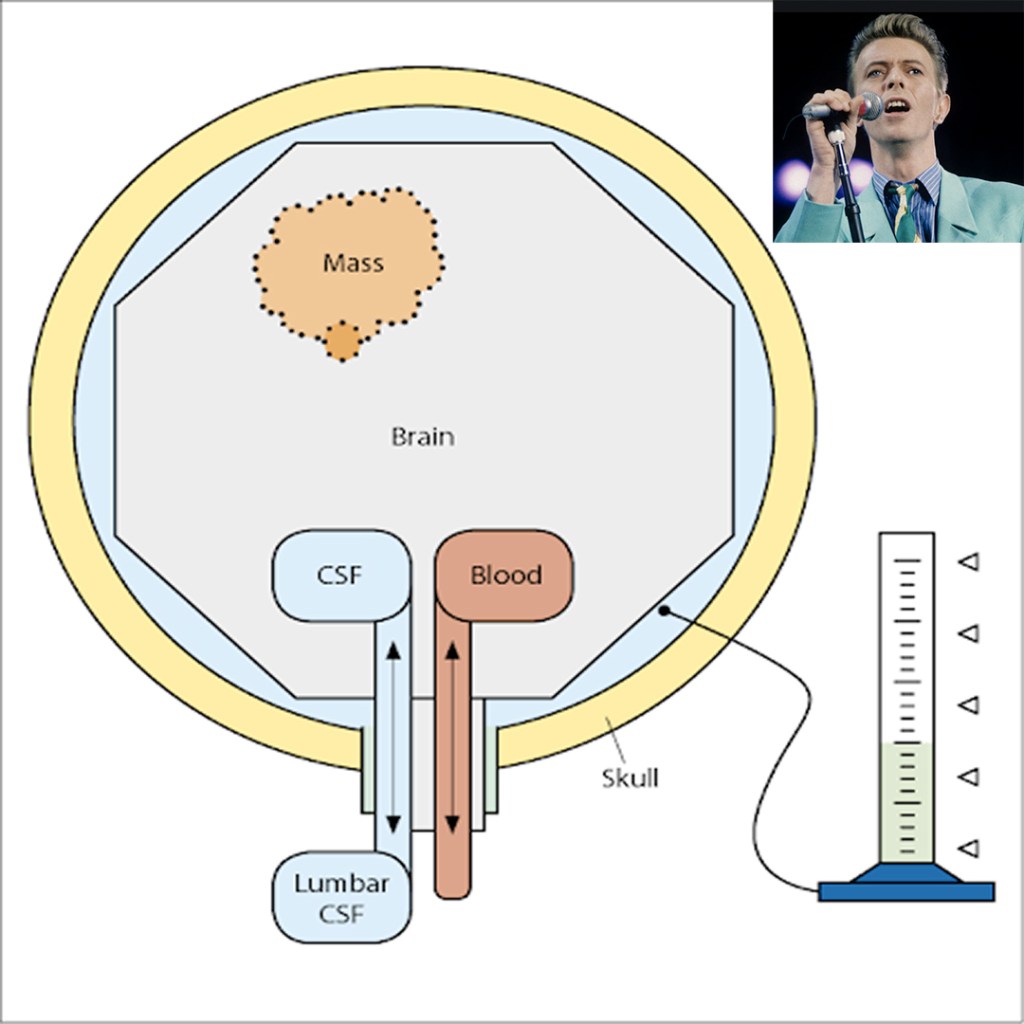
62yo man, with a history of pseudotumor cerebri, presents to your clinic with progressive headache and vision changes. You would like to confirm an increased intracranial pressure before sending him to the neurologist.
- What are two (2) ways at the bedside you can confirm and what are the thresholds for positive findings?
Answer
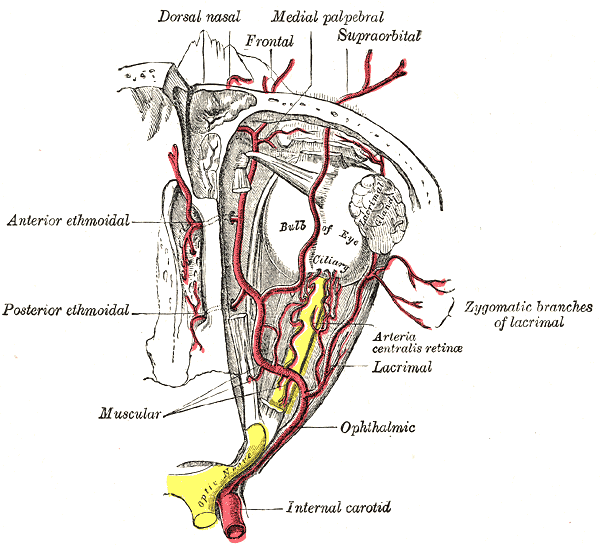
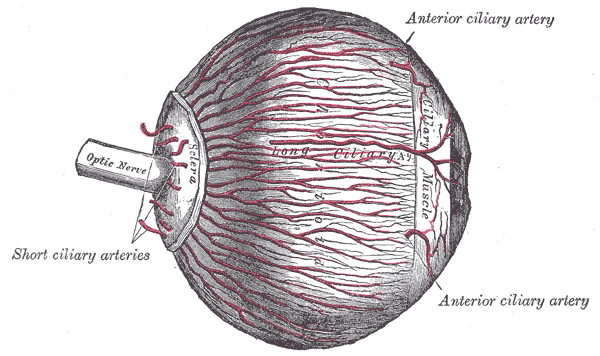
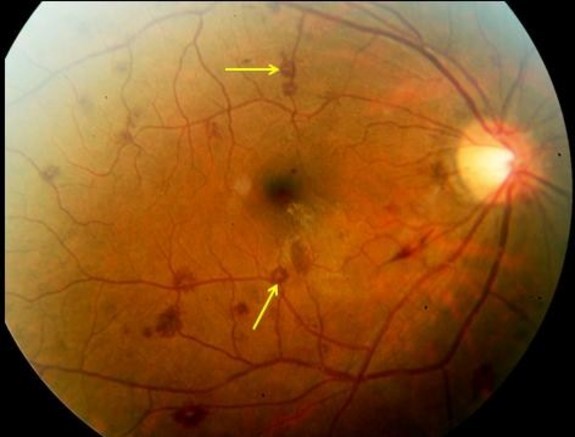
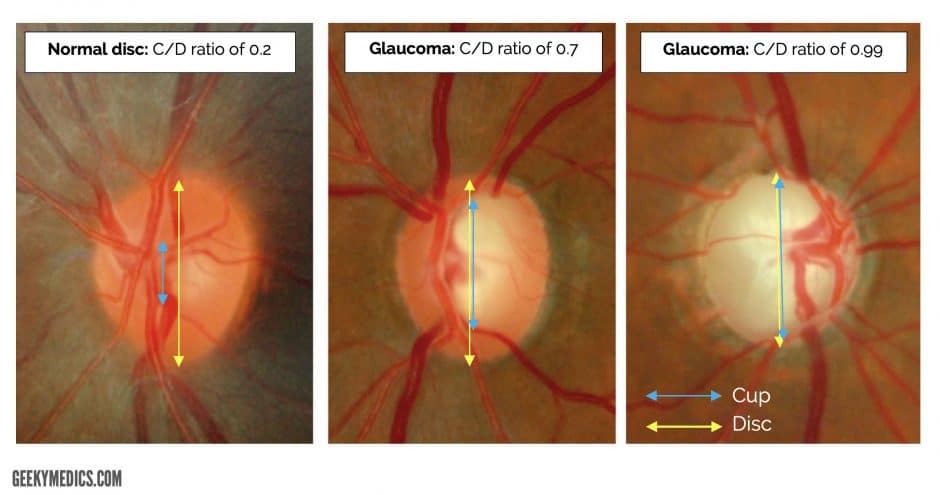
- The old and busted bedside way to determine if a patient has increased intracranial pressure is the fundoscopic examination. What you are looking for specifically is the cup:disc ratio of the optic nerve. Normal is around 0.3, or 1/3rd. If it is increased, it suggests increased intracranial pressure.
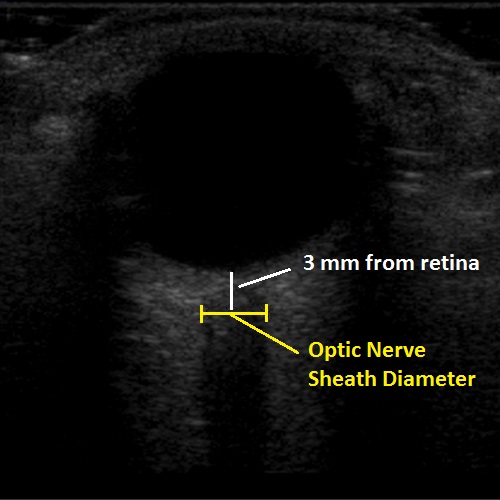
2. The new, hotness is using bedside POCUS to measure the optic nerve directly. Using the high frequency linear probe with a tegaderm placed over the patient eye, place a generous amount of gel over the globe and measure the optic nerve 3mm from the retina. A normal optic nerve should be < 5mm in diameter and anything over than suggests increased intracranial pressure