

***LISTEN TO THE PODCAST HERE***

Vector
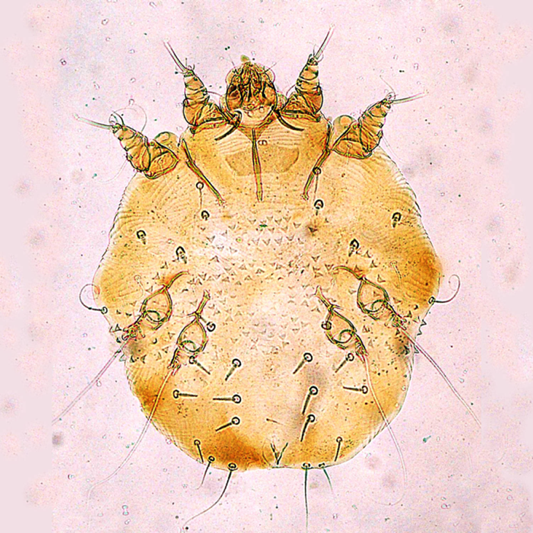
Sarcoptes scabiei
Scabies is caused by the mite Sarcoptes scabiei, which is a whitish-brown, eight-legged mite and it just barely visible by the naked eye at its largest size of 0.4×0.3mm. Only the female mite causes the dermatologic manifestations seen in scabies, as it burrows into the epidermis down to the stratum granulosum layer to lay her eggs.

The female mite can grow these burrows up to 2mm per day and lay 2-3 eggs, up to a total of 10-25 eggs. These eggs hatch after 3-4 days, molt multiple times, and burrow to the surface to mate and then return to continue this viscous cycle. Typically, incubation takes 3-6 weeks after infestations until symptoms present.
Transmission
Scabies are transmitted from direct contact with an infected person and most commonly is sexually acquired. Although not as common, transmission has also been reported to occur through contaminated clothing or bedding as these mites can survive off a host for up to 24-36 hours. Animals can contract scabies, but these rarely cause disease in humans, as they do not reproduce on human hosts.
Risk Factors
- Colder temperatures
- Higher humidity
- Crowded areas with close contact
Signs and Symptoms
The typically manifestation of scabies is an intensely pruritic rash that is worse at night. The lesions of the rash are small, erythematous, papules typically with an excoriated, hemorrhagic crust. The burrows that may be seen are thin gray/brown/red lines up to 20mm in length.


Areas most common infected are: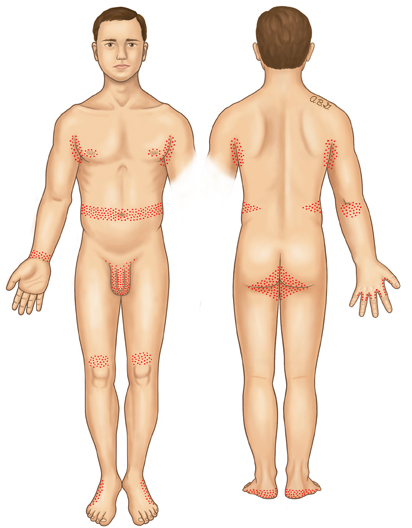
- Webs of fingers
- Flexor surface of wrist
- Extensor surface of elbow
- Axilliary folds
- Peri-areolar
- Periumbilical
- Inguinal folds
- Genital regions
- Extensor surface of knees
Head, face, and back are not commonly seen and this is theorized to be due to the increased oil production in these areas.
Crusted (Norwegian) Scabies
Immunocomprimised, eldery, debilitated, or disabled patients are at increased risk of developing this severe form of scabies. These mites are not more virulent, but because of their underlying medical conditions, the concentration of mites is much more numerous. These patients develop thick crusts and are highly contagious due to the overwhelming contamination.

Diagnosis
This should be a diagnosis of history and physical exam alone. Skin scrapings can visualize the mites or eggs under the microscope.
Dermoscopy can be used to see the mite in burrow and is classically referred to as the “delta wing” sign, which is the dark head of the mite at the end of a burrow.

“delta wing” sign
Treatment
- Topical
- Permethrin 5% cream
- Apply from jaw line to the soles of feet
- Leave overnight (8-14 hours) and washed off the next day
- May be repeated 1-2 weeks later
- Special populations
- Category B in pregnancy
- Safe in infants < 1 month
- Crusted (Norwegian)
- Daily application x 7 days, then 2x/wk until cured
- Permethrin 5% cream
- Systemic
- Ivermectin (3mg tabs)
- 2 mg/kg single dose
- Single dose not as effective as single application of permethrin
- 2nd dose, 1 week later as effective as single application of permethrin
- Recommended for large outbreaks, multiple infections in a single-household
- Not recommended in pregnancy or children < 15kg
- Crusted (Norwegian)
- 2 mg/kg/dose given on day 1, 2, 8, 9, and 15
- 2 mg/kg single dose
- Ivermectin (3mg tabs)
- Pruritus
- Hydroxyzine 25mg q6hr
- Mirtazapine 4.5-15mg qHS
- Prednisone – 2-week taper starting at 60mg/day
Prevention of Re-infestation
Recommendations are for all close-contact household members to be treated simultaneously, even if asymptomatic, to prevent cross contamination and re-infestation. Patients should be instructed to wash all clothing/bedding on the hot water cycle with high heat drying to kill any mites. Stuffed animals, jackets, or any other objects not feasible to wash, can be isolated in a plastic bag for 3 days. Fumigation is not necessary
References
- Romani L, Steer AC, Whitfeld MJ, Kaldor JM. Prevalence of scabies and impetigo worldwide: a systematic review. Lancet. Infectious diseases. 2015;15(8):960-7. [pubmed]
- Chosidow O. Clinical practices. Scabies. NEJM. 2006;354(16):1718-27. [pubmed]
- Heukelbach J, Feldmeier H. Scabies. Lancet. 2006;367(9524):1767-74. [pubmed]
- Johnston G, Sladden M. Scabies: diagnosis and treatment. BMJ. 2005;331(7517):619-22. [pubmed]
- Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. NEJM. 2010;362(8):717-25. [pubmed]
- Fuller LC. Epidemiology of scabies. Current Opinion in Infectious Diseases. 2013;26(2):123-6. [pubmed]
- Epidemiology and Risk Factors. Parasites – Scabies. Centers for Disease Control. Accessed December 14th, 2016. https://www.cdc.gov/parasites/scabies/epi.html
- Strong M, Johnstone P. Interventions for treating scabies. The Cochrane database of systematic reviews. 2007. [pubmed]
- Romani L, Whitfeld MJ, Koroivueta J. Mass Drug Administration for Scabies Control in a Population with Endemic Disease. NEJM. 2015;373(24):2305-13. [pubmed]
- Usha V, Gopalakrishnan Nair TV. A comparative study of oral ivermectin and topical permethrin cream in the treatment of scabies. Journal of the American Academy of Dermatology. 2000;42(2 Pt 1):236-40. [pubmed]
- Chambliss ML. Treating asymptomatic bodily contacts of patients with scabies. Archives of Family Medicine. 2000;9(5):473-4. [pubmed]
