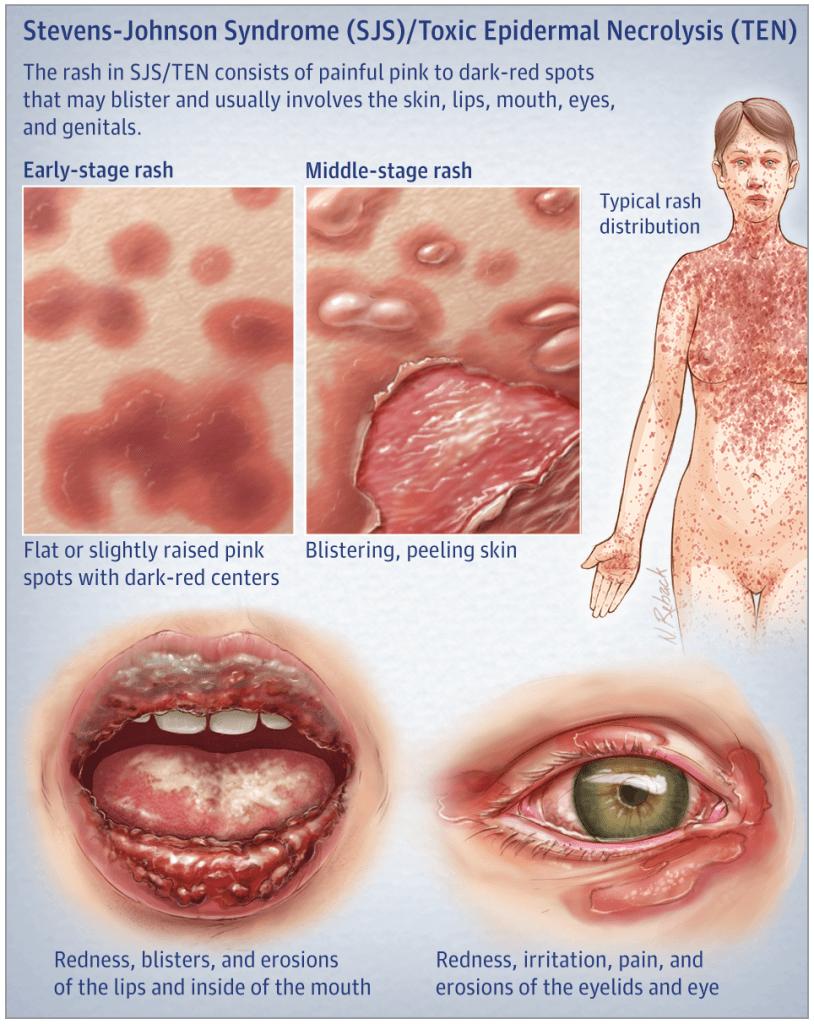
A 29yo patient is seen for a severe drug reaction after starting lamotrigine (Lamictal) for new-onset epilepsy. She has significant desquamation of her mucous membranes as well as large patches of denuded epidermis with multiple bullae present.
What is the clinically distinguishing feature between Steven-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN)?
Answer
The main clinical difference between SJS and TEN is the severity and degree of involvement. SJS classically is < 10% TBSA involvement, where as TEN is > 30% TBSA.
Definition – Exfoliation of the outermost layer and elicitation of blistering as a result of gentle mechanical pressure on the skin
Clinical Significance – This sign is classically associated with pemphigus vulgaris and is used to differentiate vulgaris (where it is present) and bullous (where it is absent). It is also present in Stevens-Johnson Syndrome, Toxic Epidermal Necrolysis, and scalded skin syndrome.
History – Named after Pyotr Vaseilyevich Nikolsky (1858-1940), who was a Russian dermatologist and received his medical doctorate from the Saint Vladimir Imperial University of Kiev in 1884. His doctoral dissertation and thesis was on pemphigus foliaceus, where he described his now famous eponym. He went on to have a career in academic medicine becoming professor at the Imperial University of Warsaw and establishing the Department of Dermatology and Venerology at the future Southern Federal University.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Grando SA, Grando AA, Glukhenky BT, Doguzov V, Nguyen VT, Holubar K. History and clinical significance of mechanical symptoms in blistering dermatoses: a reappraisal. Journal of the American Academy of Dermatology. 2003; 48(1):86-92. [pubmed]
A 29yo patient is seen for a severe drug reaction after starting lamotrigine (Lamictal) for new-onset epilepsy. She has significant desquamation of her mucous membranes as well as large patches of denuded epidermis with multiple bullae present.
What is the clinically distinguishing feature between Steven-Johnson Syndrome and Toxic Epidermal Necrolysis?
Other known aliases – Langer’s lines of skin tension, cleavage lines
Definition – topographical lines on the human body that correspond to the natural orientation of the collagen fibers of the dermis and are parallel to the orientation of the underlying muscle fibers
Clinical Significance – Incisions made on the skin that run parallel with these lines produce much less tension on the wound, heal better with less scarring, and have a much better cosmetic appearance. This is important in cosmetic surgery applications, as well as elective surgical procedures when you can select where to make your incision.
History – Named after Karl Langer (1819-1887), an Austrian anatomist, who received his medical doctorate from the Universities of Vienna and Prague. He worked under Joseph Hyrtl as a prosector for the University of Vienna and later becoming the director in 1874. In his famous procedure discovering these tension lines, he punctured circular holes on the skin of cadavers and noticed that they would result in ellipisoidal wounds. By following the direction of these ellipses, he was able to topographically map these lines on the entire body. He did give credit to Baron Dupuytren as being the first to observe this phenomenon and published his findings in 1861 entitled “Zur Anatomie und Physiologie der Haut. Über die Spaltbarkeit der Cutis”
Karl Langer
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
What are the 5 things to assess in a suspicious lesion/mole to evaluate for melanoma?
Answer
The ABCDEs of melanoma will help you identify suspicious lesions that will need dermatologic follow-up
Asymmetry
Draw a line through the lesion and the two halves do not look similar, it is concerning
Border Irregularity
If the borders of the lesion are not uniform and smooth, it is concerning
Color
Different colors within the same lesion are concerning
Diameter
≥ 6 mm is concerning
Evolution
Any lesion that changes in size, shape, color is concerning
The is also another set of criteria that was developed in the UK by the United Kingdom National Institute for Clinical Excellence (NICE) and by the Scottish Intercollegiate Guidelines Network called the Glasgow Seven-point Checklist. These guidelines incorporate 3 major and 4 minor criteria and any major or 3 minor criteria is an indication for referral.
Major
Change in size or new lesion
Change in shape
Change in color
Minor
Diameter ≥ 7mm
Inflammation
Crusting or bleeding
Sensory change
Once a patient has been referred to a dermatologist, they use a similar seven point system on dermoscopy to diagnose melanoma.
Argenziano G, Fabbrocini G, Carli P, De Giorgi V, Sammarco E, Delfino M. Epiluminescence microscopy for the diagnosis of doubtful melanocytic skin lesions. Comparison of the ABCD rule of dermatoscopy and a new 7-point checklist based on pattern analysis. Archives of dermatology. 1998; 134(12):1563-70. [pubmed]
Other Known Aliases – Ultraviolet (UV)-A lamp, blacklight
Definition – Handheld UV light that emits UV-A (long-wave) light with a violet filter, which blocks most of the visible light, and only allows the UV-A through
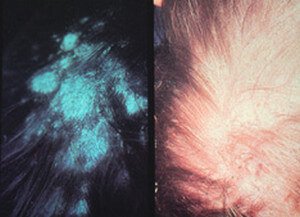
Clinical Significance – There are many medical applications for using UV light for quick, bedside diagnosis. One of these is for fungal infections of the skin, most commonly Tinea infections. Tinea infections will fluoresce under UV-A light.
Tinea versicolor
Tinea capitis
History –Named after Robert W. Wood (1868-1955), who was an American physicist, inventor, and a pioneer in infrared and ultraviolet photography. In 1903, he developed a filter that would block visible light, but be transparent to both infrared and ultraviolet light. He won several awards and honors in the field of optics (he even has a crater on the moon named after him) and is the namesake of the R.W. Wood Prize of the Optical Society of America, which recognizes outstanding discovery, achievement, or invention.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Ponka D, Baddar F. Wood lamp examination. Canadian family physician Medecin de famille canadien. 2012; 58(9):976. [pubmed]
Ducharme EE, Silverberg NB. Selected applications of technology in the pediatric dermatology office. Seminars in cutaneous medicine and surgery. 2008; 27(1):94-100. [pubmed]
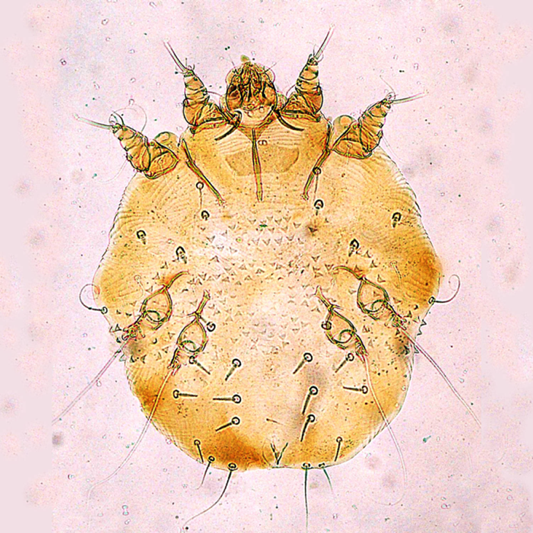
Scabies is caused by the mite Sarcoptes scabiei, which is a whitish-brown, eight-legged mite and it just barely visible by the naked eye at its largest size of 0.4×0.3mm. Only the female mite causes the dermatologic manifestations seen in scabies, as it burrows into the epidermis down to the stratum granulosum layer to lay her eggs.
The female mite can grow these burrows up to 2mm per day and lay 2-3 eggs, up to a total of 10-25 eggs. These eggs hatch after 3-4 days, molt multiple times, and burrow to the surface to mate and then return to continue this viscous cycle. Typically, incubation takes 3-6 weeks after infestations until symptoms present.
Transmission
Scabies are transmitted from direct contact with an infected person and most commonly is sexually acquired. Although not as common, transmission has also been reported to occur through contaminated clothing or bedding as these mites can survive off a host for up to 24-36 hours. Animals can contract scabies, but these rarely cause disease in humans, as they do not reproduce on human hosts.
Risk Factors
Colder temperatures
Higher humidity
Crowded areas with close contact
Signs and Symptoms
The typically manifestation of scabies is an intensely pruritic rash that is worse at night. The lesions of the rash are small, erythematous, papules typically with an excoriated, hemorrhagic crust. The burrows that may be seen are thin gray/brown/red lines up to 20mm in length.
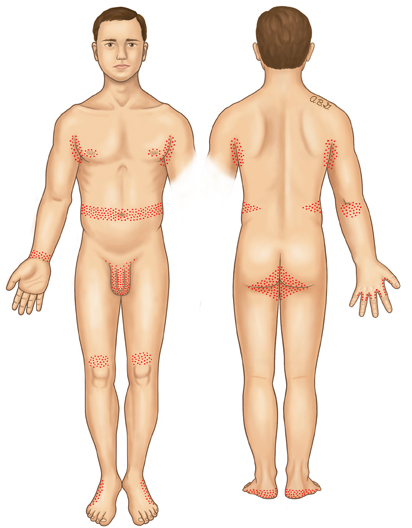
Areas most common infected are:
Webs of fingers
Flexor surface of wrist
Extensor surface of elbow
Axilliary folds
Peri-areolar
Periumbilical
Inguinal folds
Genital regions
Extensor surface of knees
Head, face, and back are not commonly seen and this is theorized to be due to the increased oil production in these areas.
Crusted (Norwegian) Scabies
Immunocomprimised, eldery, debilitated, or disabled patients are at increased risk of developing this severe form of scabies. These mites are not more virulent, but because of their underlying medical conditions, the concentration of mites is much more numerous. These patients develop thick crusts and are highly contagious due to the overwhelming contamination.
Diagnosis
This should be a diagnosis of history and physical exam alone. Skin scrapings can visualize the mites or eggs under the microscope.
Dermoscopy can be used to see the mite in burrow and is classically referred to as the “delta wing” sign, which is the dark head of the mite at the end of a burrow.
“delta wing” sign
Treatment
Topical
Permethrin 5% cream
Apply from jaw line to the soles of feet
Leave overnight (8-14 hours) and washed off the next day
May be repeated 1-2 weeks later
Special populations
Category B in pregnancy
Safe in infants < 1 month
Crusted (Norwegian)
Daily application x 7 days, then 2x/wk until cured
Systemic
Ivermectin (3mg tabs)
2 mg/kg single dose
Single dose not as effective as single application of permethrin
2nd dose, 1 week later as effective as single application of permethrin
Recommended for large outbreaks, multiple infections in a single-household
Not recommended in pregnancy or children < 15kg
Crusted (Norwegian)
2 mg/kg/dose given on day 1, 2, 8, 9, and 15
Pruritus
Hydroxyzine 25mg q6hr
Mirtazapine 4.5-15mg qHS
Prednisone – 2-week taper starting at 60mg/day
Prevention of Re-infestation
Recommendations are for all close-contact household members to be treated simultaneously, even if asymptomatic, to prevent cross contamination and re-infestation. Patients should be instructed to wash all clothing/bedding on the hot water cycle with high heat drying to kill any mites. Stuffed animals, jackets, or any other objects not feasible to wash, can be isolated in a plastic bag for 3 days. Fumigation is not necessary
References
Romani L, Steer AC, Whitfeld MJ, Kaldor JM. Prevalence of scabies and impetigo worldwide: a systematic review. Lancet. Infectious diseases. 2015;15(8):960-7. [pubmed]
Chosidow O. Clinical practices. Scabies. NEJM. 2006;354(16):1718-27. [pubmed]
Heukelbach J, Feldmeier H. Scabies. Lancet. 2006;367(9524):1767-74. [pubmed]
Johnston G, Sladden M. Scabies: diagnosis and treatment. BMJ. 2005;331(7517):619-22. [pubmed]
Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. NEJM. 2010;362(8):717-25. [pubmed]
Fuller LC. Epidemiology of scabies. Current Opinion in Infectious Diseases. 2013;26(2):123-6. [pubmed]
Strong M, Johnstone P. Interventions for treating scabies. The Cochrane database of systematic reviews. 2007. [pubmed]
Romani L, Whitfeld MJ, Koroivueta J. Mass Drug Administration for Scabies Control in a Population with Endemic Disease. NEJM. 2015;373(24):2305-13. [pubmed]
Usha V, Gopalakrishnan Nair TV. A comparative study of oral ivermectin and topical permethrin cream in the treatment of scabies. Journal of the American Academy of Dermatology. 2000;42(2 Pt 1):236-40. [pubmed]
Chambliss ML. Treating asymptomatic bodily contacts of patients with scabies. Archives of Family Medicine. 2000;9(5):473-4. [pubmed]