
***LISTEN TO THE PODCAST HERE***
Epidemiology
Small bowel obstruction (SBO) is one of the more common surgical emergencies in US, due to the increased intraluminal pressures which can lead to intestinal ischemia and risk of spontaneous rupture. Overall mortality increases significantly if either of these occur. It is estimated that over 300,000 surgeries per year occur in the US for bowel obstructions, with the small bowel making up around 80%. Although it can happen at age, there is a higher trend to older patients and thee is equal incidence with both genders.
Risk Factors
The most common cause of SBO is postoperative adhesions, but there are numerous other causes that you should keep on your differential.

Signs and Symptoms
- Abdominal pain
- Paroxysms of periumbilical pain (3-5 minutes)
- Nausea
- Vomiting
- Obstipation
Physical Examination
- Dehydration
- Tachycardia, orthostasis, decreased urine output
- +/- Distension
- Changes in bowel sounds
- Hyperactive à muffled à absent
- Percussion changes
- Tympanic with distension
- Dullness with fluid
- Peritoneal signs if perforation present
- +/- hemoccult
Laboratory Studies
- CBC with differential
- Anemia can point to a chronic condition
- BMP
- ABG
- Acidosis = bowel ischemia, volume depletion
- Alkalosis = vomiting
- Serum lactate
Imaging Studies
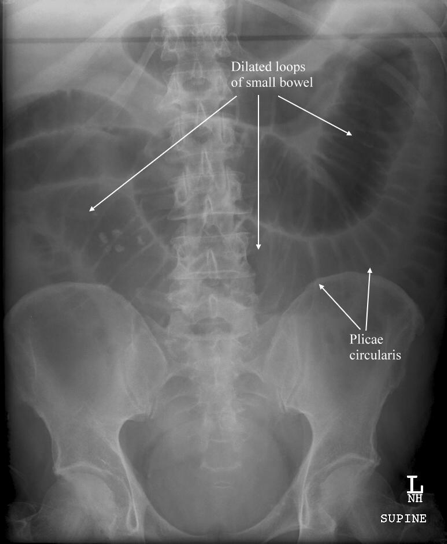
- Plain Radiographs
- Dilated loops of small bowel with air/fluid levels on upright film
- May also see a paucity of gas in distal intestines

-
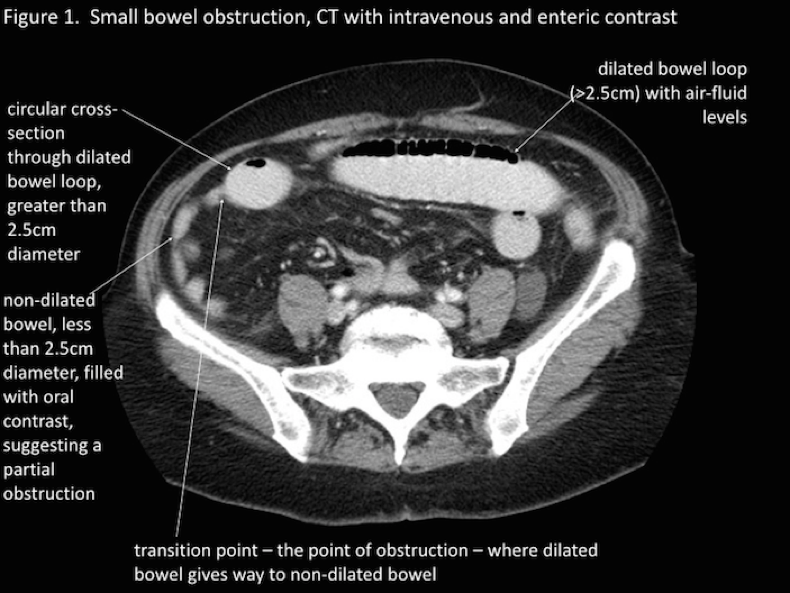
Small bowel dilation ≥ 2.5cm is diagnostic

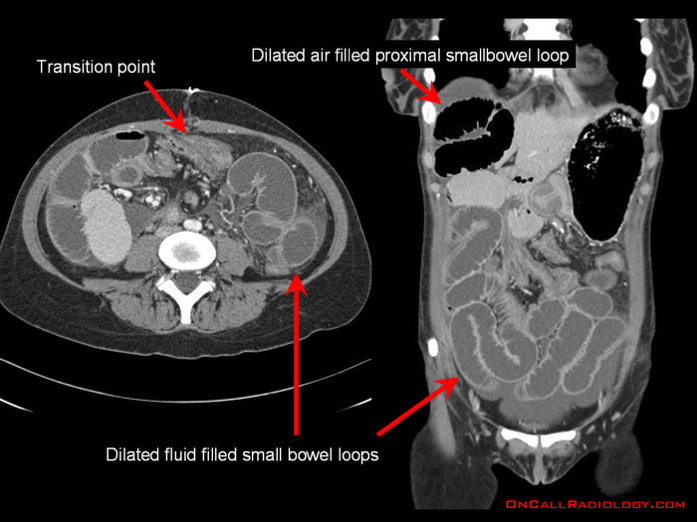
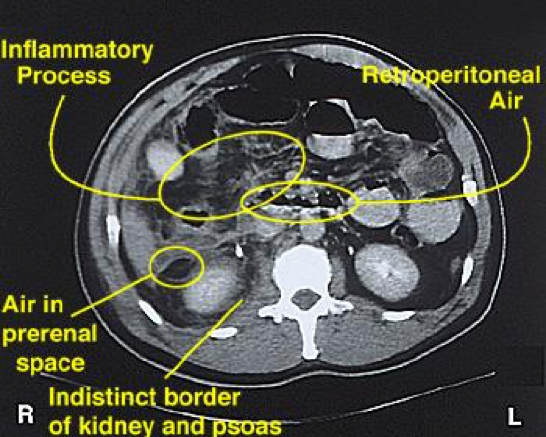
- Abdominal CT
- Much more sensitive and can also identify the specific causes
- Can also identify a transition point


- Other radiological signs on CT consistent with SBO include:
- Bowel wall thickening > 3mm
- Submucosal edema
- Mesenteric edema
- Ascites
- Target sign (intussusception)
- Whirl sign (volvulus)
- Venous cut-off sign (thrombosis)
- Ultrasound
- Not as good as CT, but better than plain radiography
- Special Considerations on Radiography
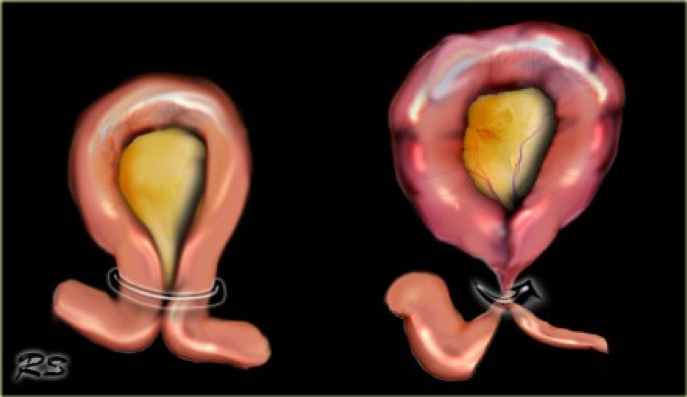
- Closed-Loop Obstruction
- High risk for ischemia, perforation, and ischemic bowel

- Ischemia and Perforation
- Closed-Loop Obstruction


Management
- Initial
- NPO
- Fluid resuscitation
- Surgery consultation
- Gastrointestinal decompression
- Not in EVERY patient, but good for patients with significant distension, nausea, and/or vomiting
- Surgery
- Nonspecific signs of bowel ischemia:
- Fever
- Leukocytosis
- Tachycardia
- Continuous and/or worsening abdominal pain
- Metabolic acidosis
- Peritonitis
- High likelihood of bowel resection if ≥ 3 of the following:
- Pain > 4 days
- Abdominal guarding on exam
- Elevated CRP > 75 mg/dL
- Leukocytosis > 10,000
- > 500cc fluid of intraabdominal fluid
- Reduced wall contrast enhancement on CT
-
- Nonspecific signs of bowel ischemia:
- Observation
- If no high-risk surgical signs present, observation with serial examinations may be used for 12-24 hours in patients with:
- Early postoperative obstruction
- Inflammatory bowel disease
- Gallstone ileus
- Infectious small bowel disease
- Colonic diverticular disease
- Exploration should proceed if no improvement
- If no high-risk surgical signs present, observation with serial examinations may be used for 12-24 hours in patients with:
References
- Miller G, Boman J, Shrier I, Gordon PH. Etiology of small bowel obstruction. American Journal of Surgery. 2000; 180(1):33-6. [pubmed]
- Markogiannakis H, Messaris E, Dardamanis D. Acute mechanical bowel obstruction: clinical presentation, etiology, management and outcome. World Journal of Gastroenterology. 2007; 13(3):432-7. [pubmed]
- Scott FI, Osterman MT, Mahmoud NN, Lewis JD. Secular trends in small-bowel obstruction and adhesiolysis in the United States: 1988-2007. American Journal of Surgery. 2012; 204(3):315-20. [pubmed]
- Drożdż W, Budzyński P. Change in mechanical bowel obstruction demographic and etiological patterns during the past century: observations from one health care institution. Archives of Surgery (Chicago, Ill. : 1960). 2012; 147(2):175-80. [pubmed]
- Taylor MR, Lalani N. Adult small bowel obstruction. Academic Emergency Medicine. 2013; 20(6):528-44. [pubmed]
- Jackson PG, Raiji MT. Evaluation and management of intestinal obstruction. American Family Physician. 2011; 83(2):159-65. [pubmed]
- Mullan CP, Siewert B, Eisenberg RL. Small bowel obstruction. American Journal of Roentgenology. 2012; 198(2):W105-17. [pubmed]
- Suri S, Gupta S, Sudhakar PJ, Venkataramu NK, Sood B, Wig JD. Comparative evaluation of plain films, ultrasound and CT in the diagnosis of intestinal obstruction. Acta radiologica. 1999; 40(4):422-8. [pubmed]
- Zalcman M, Sy M, Donckier V, Closset J, Gansbeke DV. Helical CT signs in the diagnosis of intestinal ischemia in small-bowel obstruction. American Journal of Roentgenology. 2000; 175(6):1601-7. [pubmed]
- Eltarawy IG, Etman YM, Zenati M, Simmons RL, Rosengart MR. Acute mesenteric ischemia: the importance of early surgical consultation. The American Surgeon. 2009; 75(3):212-9. [pubmed]
- Schwenter F, Poletti PA, Platon A, Perneger T, Morel P, Gervaz P. Clinicoradiological score for predicting the risk of strangulated small bowel obstruction. The British Journal of Surgery. 2010; 97(7):1119-25. [pubmed]
