*** LISTEN TO THE PODCAST HERE ***




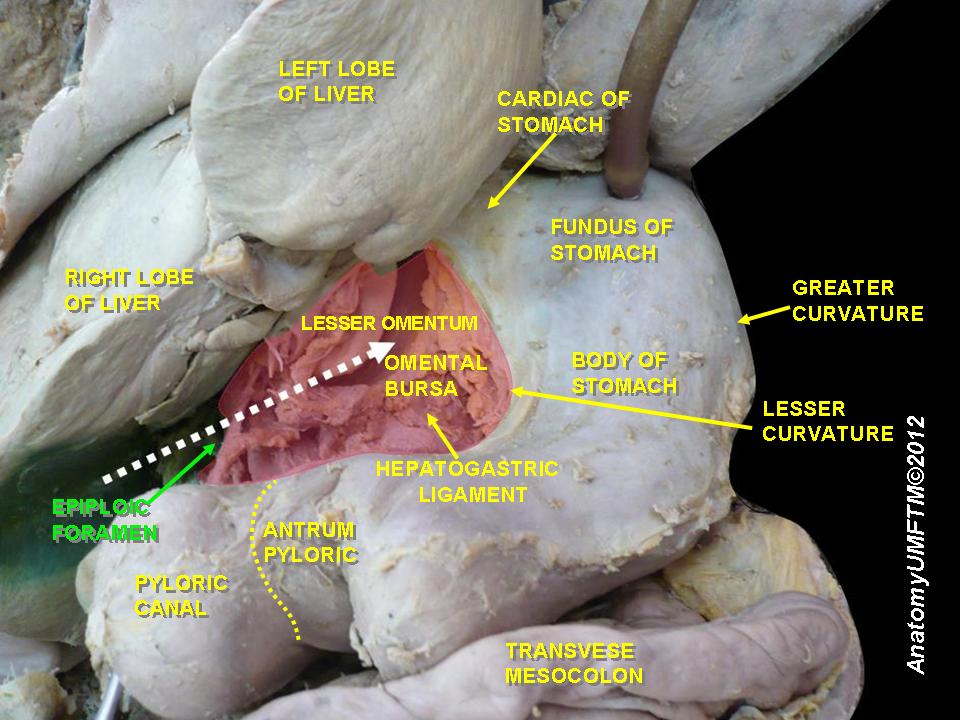
Foramen of Winslow
Other Known Aliases – omental foramen, epiploic foramen
Definition – anatomic passage between the greater sac and the lesser sac of the abdomen
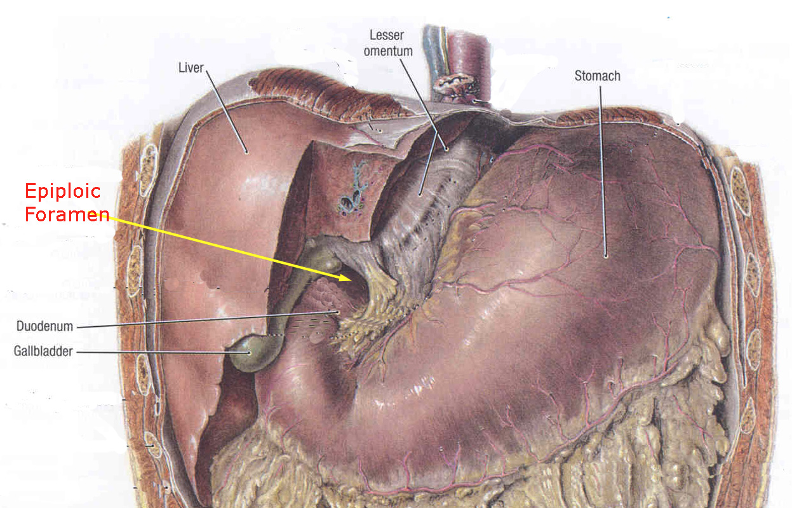
Clinical Significance – there are four anatomic borders of this communication:
History – Named after Jacob Winslow (1669-1760), a Danish-born French anatomist who received his degree from Ole Borch’s College in 1693, while training under barber-surgeon Johannes de Buchwalde. He would concentrate on anatomy, instead of surgery, as the site of blood “alarmed him”. He would go on to train with many of the most revered surgeons and anatomists of his time while traveling Europe and was widely regarded as the greatest European anatomist of his day. His career would culminate in achieving professor anatomicus and full professor of anatomy at Jardin du Roi in 1743. His most famous work entitled “Exposition anatomique de la structure du corps humain” was published in 1732 and was the quintessential anatomical text of the mid-1700’s


References

Question
A 37yo man is presenting to your practice to establish primary care. He reports a history of controlled inflammatory bowel disease and sees a gastroenterologist every 6 months. Before you begin your physical examination:
Answer
A simple mnemonic for the extraintestinal manifestations of inflammatory bowel disease is A PIE SACK:

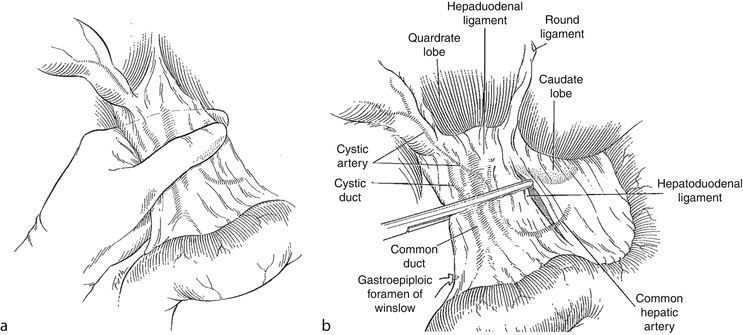
Pringle Maneuver
Other Known Aliases – none
Definition – surgical technique whereby the hepatoduodenal ligament is clamped to limit blood flow through the hepatic artery and portal vein to the liver

Clinical Significance – the specific technique is to insert an index finger through the foramen of Winslow behind the porta hepatis and pinch between the finger and the thumb. You can also slide a non-crushing clamp along the finger, or wrap a vessel loop around to occlude. This technique controls the majority of the blood flow to the liver and is used to control bleeding during liver surgery or after liver trauma.
History – Named after James Hogarth Pringle (1863-1941), who was an Australian/Scottish surgeon and received his medical doctorate from the University of Edinburgh Medical School in 1885. He would have a prestigious career pioneering management and treatments for long bone fractures, head injuries, malignant melanomas, and reconstructive arterial surgery using vein grafts. He would describe his eponymous maneuver in 1908 in an article in the Annals of Surgery entitled “Notes on the Arrest of Hepatic Hemorrhage Due to Trauma”. It should also be noted that he was a fervent advocate for women in medicine, allowing them in his clinic well before any of his colleagues, and becoming Lecturer in Surgery and Demonstrator of Anatomy at Queen Margaret College, which was one of the first medical schools for women in Scotland.


References
Question
A 37yo man is presenting to your practice to establish primary care. He reports a history of controlled inflammatory bowel disease and sees a gastroenterologist every 6 months. Before you begin your physical examination:

Triangle of Calot
Other Known Aliases – none
Definition – anatomic space bordered by the cystic duct (inferiorly), common hepatic duct (medially) and cystic artery (superiorly)

Clinical Significance – this anatomic space is where you can see lymphadenopathy in patients with cholecystitis. This is often confused with the cystohepatic triangle (read more here).
History – Named after Jean-François Calot (1861-1944), who was a French surgeon and received his medical doctorate from Saine-Pe de Bigorre in 1880. He would go on to have a modest career in the field of orthopaedic surgery, and is known for describing the treatment of spinal deformities in Pott’s Disease. He would describe his eponymonic area in his doctoral thesis defense in 1891.

References
***LISTEN TO THE PODCAST HERE***






Puestow Procedure
Other Known Aliases – Puestow-Gillesby procedure, lateral pancreaticojejunostomy
Definition – side-to-side anastomosis of the main pancreatic duct of Wirsung to the proximal jejunum

Clinical Significance – this is a surgical management option for patients with chronic pancreatitis by simultaneously facilitating drainage and preserving physiologic function of the pancreas.
History – Named after Charles Bernard Puestow (1902-1973), an American surgeon who recieved his medical doctorate from the University of Pennsylvania in 1925. He would serve as a military surgeon during the 2nd World War and commanded the 27th Evacuation Hospital providing surgical services to wounded soldiers in Europe and North Africa. His commitment to the veteran population would continue after the war when he established the first surgical residency program based in a veterans hospitals in the United States in 1946. It was at Hines Veterans Hospital in Illinois where he and his partner, William Gillesby, would publish their experience and outcomes on 21 patients with chronic pancreatitis in 1958, which would lead to the creation of his eponymonic surgical procedure.

References
Question
Surgery is a major physiologic stress and often is accompanied by biochemical derangements that effect homeostasis in the post-operative period. Describe the most common clinical scenarios that can cause each of the four main acid-base imbalances in a post-surgical patient.
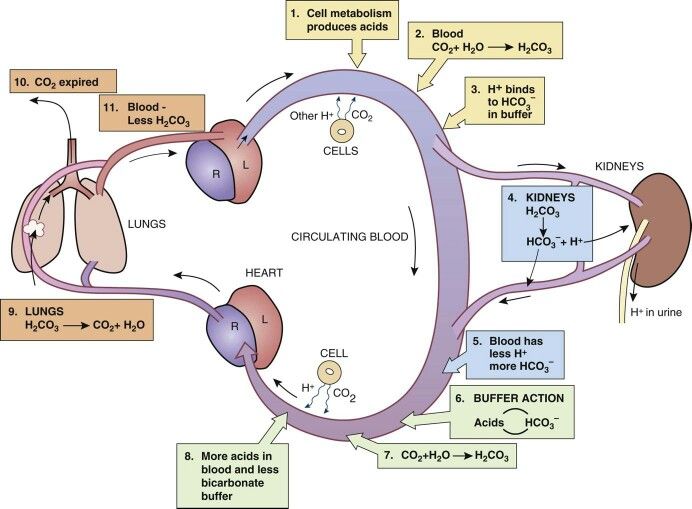
Answer


