
***LISTEN TO THE PODCAST HERE***
Definitions
- Dyspepsia
- Upper abdominal pain or discomfort
- Gastritis
- Epithelial or endothelial damage with histologic evidence of inflammation
- 2 types
- Gastric
- Duodenal
Epidemiology
- Annual incidence in developed countries 0.1-0.19%, or 0.7 cases per 1000 person-years
- Lifetime prevalence of PUD in 10-20% in pylori (+) patients vs 5-10% in H.pylori (-) patients
- Increases with age
- 13x higher risk of bleeding in patients > 70yo
- More common in males
- Differences between Gastric and Duodenal Ulcers
- DU occur up to 20 years before GU
- DU 5x more common than GU
Etiologies
There are numerous causes of PUD and include infections, stress, medications, alcohol, cirrhosis, neoplasms, etc. The two main causes in developed countries are:
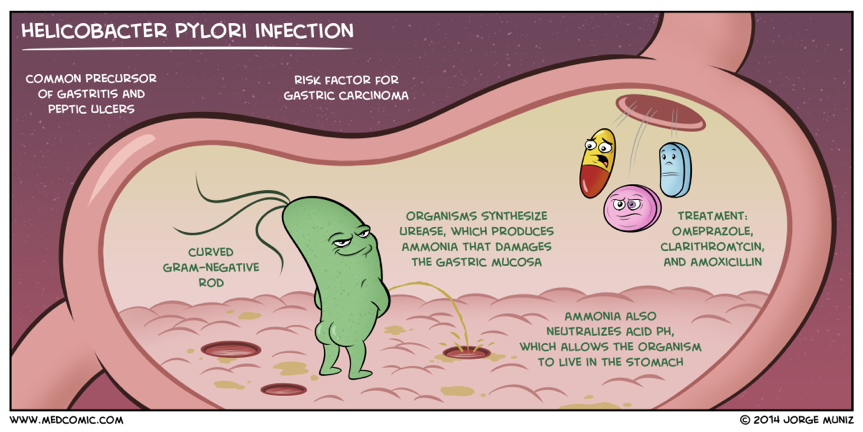
- Helicobacter pylori
- Spiral gram negative rod
- Decreasing incidence due to better hygiene, OTC medications, and antibiotic use

- Non-Steroidal Antiflammatory Drugs (NSAIDs)
- 1-4% per year risk of PUD
- Risk factors
- Prior history of PUD or pylori infection
- Dose
- Duration
- Age > 75 years
- Co-therapy
- Corticosteroids, anticoagulants, SSRI, bisphosphonates, antiplatelets


Clinical Manifestations
- Up to 70% of peptic ulcers are asymptomatic
- Present later with complications
- Up to 80% present with bleeding without preceding symptoms
- Dyspepsia is the most common symptoms
- May also have radiation to the back
- Relation to food intake
- GU – Worse
- DU – Better
- Night symptoms
- GU – 1/3 of patients
- DU – 2/3 of patients
- Nausea, vomiting, anorexia, early satiety, epigastric fullness

Complications
- Bleeding
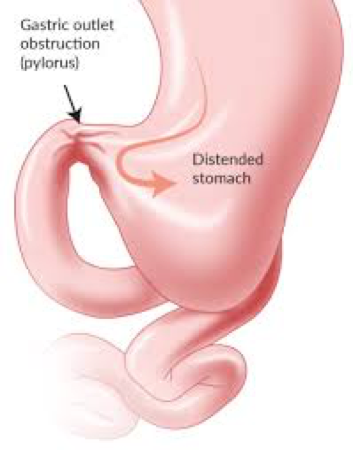
- Gastric Outlet Obstruction
- Penetration
- Change in typical symptoms

- Perforation
- 2-10% perforation rate
- Duodenal – 60%
- Antrum – 20%
- Gastric Body – 20%

- 2-10% perforation rate


Red Flags
Work-up
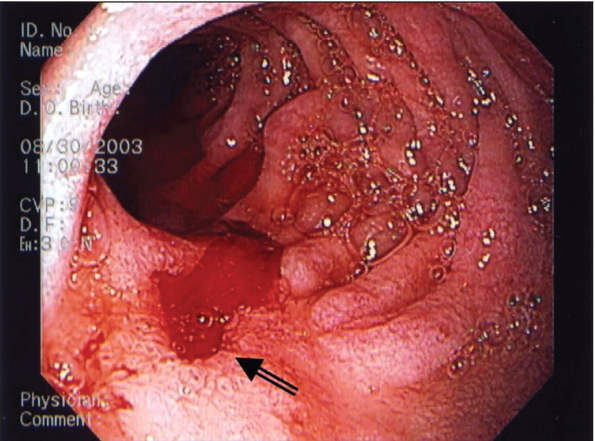
- Endoscopy
- Up to 90% sensitivity in identifying ulcer
- Next step if any red flags
- Malignant features requiring biopsy:
- Ulcerated mass protruding from lumen
- Nodular, clubbed, or fused folds
- Overhanging, irregular, or thickened ulcer margins
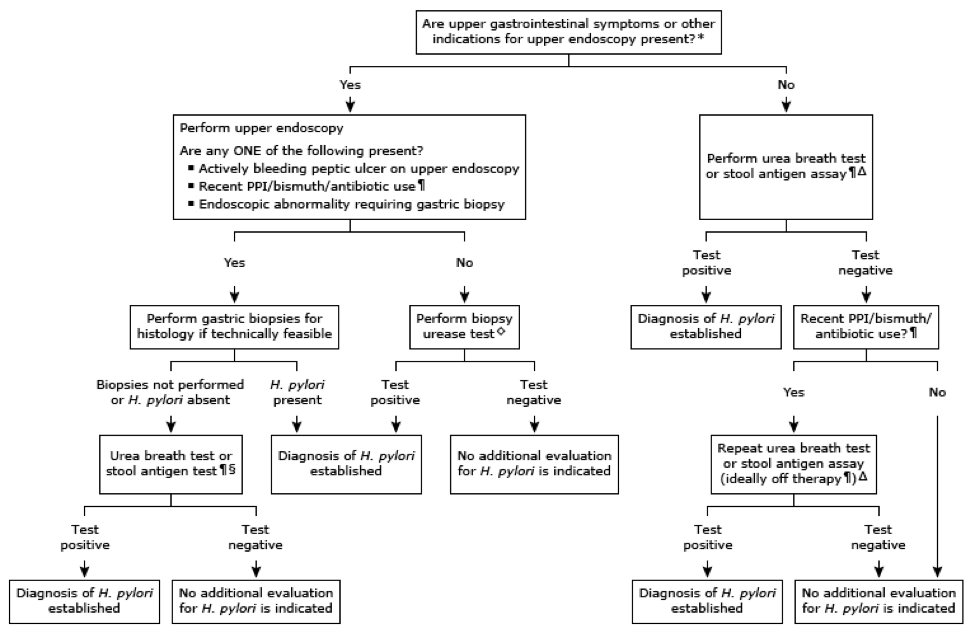
- H/pylori Testing
- pylori serology and stool antigen testing
- May be falsely negative if on concurrent PPI
- Biopsy testing and histology from endoscopy
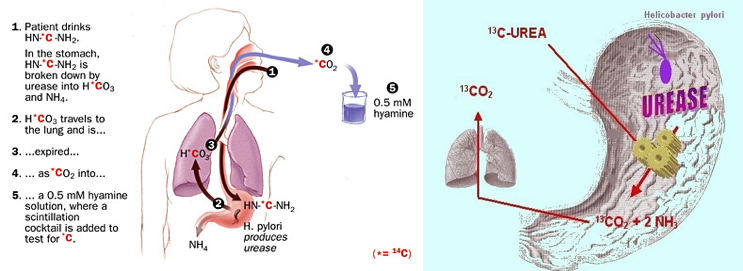
- Urea Breath Test
- pylori serology and stool antigen testing
Initial Management
- Withdrawal of offending or contributing factors
- Stop NSAIDs, smoking, EtOH, precipitant foods
- Antisecretory therapy
- (+) H. pylori Ulcer
- Uncomplicated – 14 days
- Complicated – up to 12 weeks
- NSAID Induced
- If stopping – 8 weeks
- If continuing – indefinitely
- Non-H.pylori, non-NSAID Ulcer
- 4-8 weeks
- PPIs out perform H2A
- Esomeprazole (Nexium) – 20-40mg daily
- Lansoprazole (Prevacid) – 15-30mg daily
- Omeprazole (Prilosec) – 20-40mg daily
- Pantoprazole (Protonix) – 20-40mg daily
- High Risk Groups Requiring Indefinite Prophylaxis
- > 2 cm ulcer on endoscopy and age > 50yo
- Refractory H. pylori negative, NSAID negative ulcer
- Failure to eradicate H. pylori
- Frequently recurrent peptic ulcers (> 2 cases in 1 one)
- Continued NSAID use
- (+) H. pylori Ulcer
- H. pylori Eradication
- Risk factors for Macrolide resistance
- Prior exposure to macrolide therapy
- ≥ 15% clarithromycin local resistance rates
- < 85% eradication rates with clarithromycin triple therapy
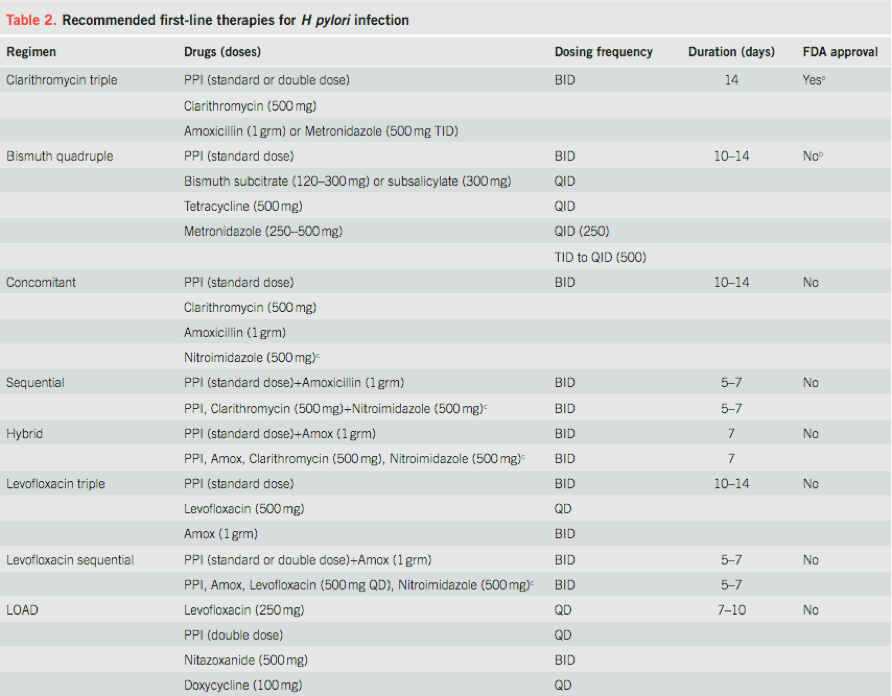
- Initial Therapy
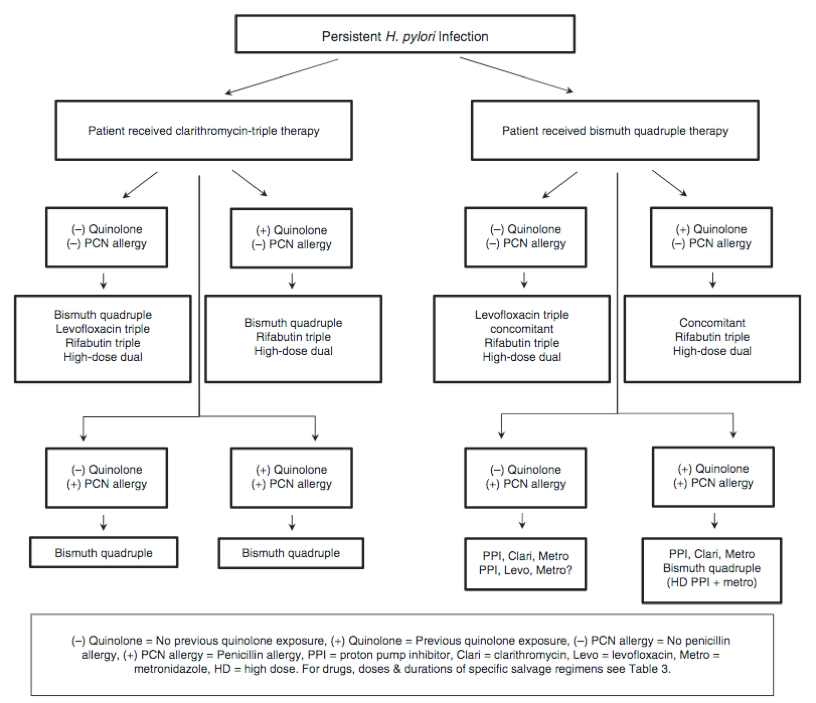
- Salvage Therapy
- 20% of patients will fail initial H. pylori eradication


- Risk factors for Macrolide resistance


References
- Sung JJ, Kuipers EJ, El-Serag HB. Systematic review: the global incidence and prevalence of peptic ulcer disease. Alimentary pharmacology & therapeutics. 2009; 29(9):938-46. [pubmed]
- Lin KJ, García Rodríguez LA, Hernández-Díaz S. Systematic review of peptic ulcer disease incidence rates: do studies without validation provide reliable estimates? Pharmacoepidemiology and drug safety. 2011; 20(7):718-28. [pubmed]
- Sonnenberg A. Temporal trends and geographical variations of peptic ulcer disease. Alimentary pharmacology & therapeutics. 1995; 9 Suppl 2:3-12. [pubmed]
- Thorat MA, Cuzick J. Prophylactic use of aspirin: systematic review of harms and approaches to mitigation in the general population. European journal of epidemiology. 2015; 30(1):5-18. [pubmed]
- García Rodríguez LA, Hernández-Díaz S. Risk of uncomplicated peptic ulcer among users of aspirin and nonaspirin nonsteroidal antiinflammatory drugs. American journal of epidemiology. 2004; 159(1):23-31. [pubmed]
- Gururatsakul M, Holloway RH, Talley NJ, Holtmann GJ. Association between clinical manifestations of complicated and uncomplicated peptic ulcer and visceral sensory dysfunction. Journal of gastroenterology and hepatology. 2010; 25(6):1162-9. [pubmed]
- Wilcox CM, Clark WS. Features associated with painless peptic ulcer bleeding. The American journal of gastroenterology. 1997; 92(8):1289-92. [pubmed]
- Paimela H, Paimela L, Myllykangas-Luosujärvi R, Kivilaakso E. Current features of peptic ulcer disease in Finland: incidence of surgery, hospital admissions and mortality for the disease during the past twenty-five years. Scandinavian journal of gastroenterology. 2002; 37(4):399-403. [pubmed]
- Malfertheiner P, Megraud F, O’Morain CA. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. 2017; 66(1):6-30. [pubmed]
- Chiorean MV, Locke GR, Zinsmeister AR, Schleck CD, Melton LJ. Changing rates of Helicobacter pylori testing and treatment in patients with peptic ulcer disease. The American journal of gastroenterology. 2002; 97(12):3015-22. [pubmed]
- Yeomans ND, Tulassay Z, Juhász L. A comparison of omeprazole with ranitidine for ulcers associated with nonsteroidal antiinflammatory drugs. Acid Suppression Trial: Ranitidine versus Omeprazole for NSAID-associated Ulcer Treatment (ASTRONAUT) Study Group. The New England journal of medicine. 1998; 338(11):719-26. [pubmed]
- Duck WM, Sobel J, Pruckler JM. Antimicrobial resistance incidence and risk factors among Helicobacter pylori-infected persons, United States. Emerging infectious diseases. 2004; 10(6):1088-94. [pubmed]
- Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. The American journal of gastroenterology. 2017; 112(2):212-239. [pubmed]
