

***LISTEN TO THE PODCAST HERE***
Pathophysiology
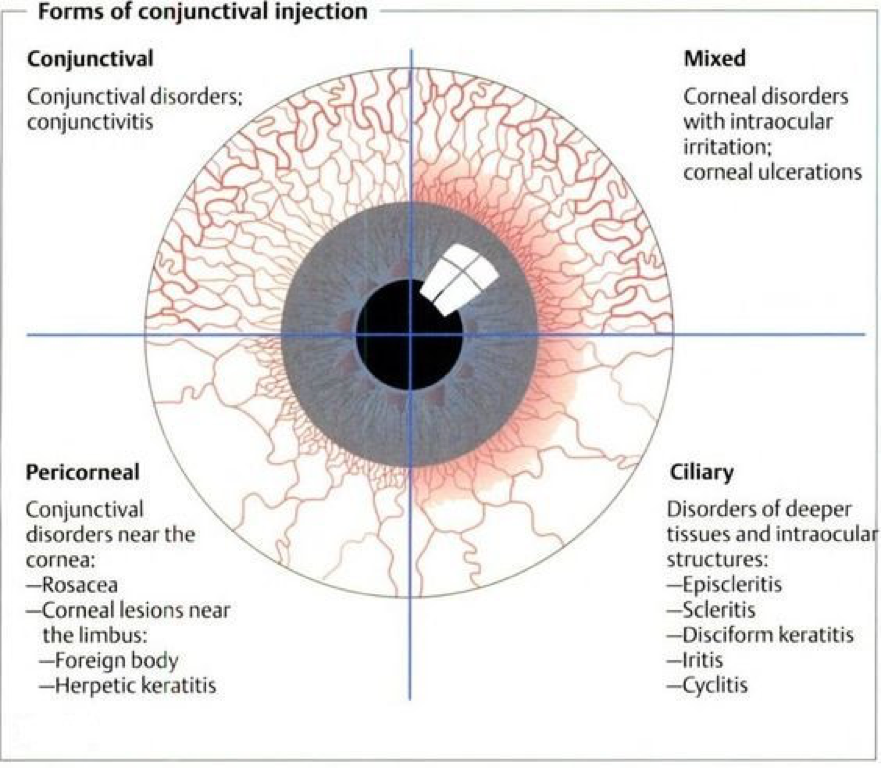
The conjunctiva is a mucous membrane that that lines the surface of the eyelids (palpebral) and globe up to the limbus (bulbar).

The conjunctiva itself is made up of non-keratinized squamous epithelium with goblet cells and substantia propria, which is highly vascularized.

The important thing to remember is that the conjunctiva is transparent, unless inflamed (which is termed “injected”).
Bacterial Conjunctivitis

- Bacterial conjunctivitis is more common in children than adults (though viral is most common overall).
- Transmission is spread from direct contact with infected drainage or contaminated objects
- Pathogens
- S. aureus, S. pneumoniae, H. influenza, M. catarrhalis
- Signs and Symptoms
- Redness and drainage in one eye
- Matted shut in the morning
- Drainage
- Continues throughout the day
- Thick and purulent
- Special Concerns
- Neisseria gonorrhoeae
- Concurrent STI symptoms
- Rapid onset of symptoms (< 12 hours)
- More pain and tenderness with marked chemosis and lymphadenopathy
- Admission with emergency ophthalmology evaluation
- Keratitis and perforation may occur
- Neisseria gonorrhoeae
Viral Conjunctivitis

- Most common cause of acute conjunctivitis
- Highly contagious and is spread through direct contact with drainage or contaminated objects
- Pathogens
- Adenovirus is the most common
- Viral prodrome
- Fever, adenopathy, pharyngitis, URI, conjunctivitis
- Drainage
- Watery, mucoserous drainage
- Matted/thick in the morning with scant, watery drainage throughout the day
- Corneal injection with burning/gritty sensation
- Starts unilateral and spreads to contralateral eye within 48 hours of symptoms onset
- Follicular pattern on palpebral conjunctiva

- Self-limiting process
- Worsens for 3-5 days with gradual resolution over the next 7-10 days

Allergic Conjunctivitis

- Caused by airborne allergens that initiate an IgE-mediated local response with mast cell degranulation and release of histamine
- Drainage
- Watery and stringy
- Signs and Symptoms
- Bilateral eye involvement
- Periorbital edema
- Allergic symptoms
- Sneezing, coughing, rash, sore throat
- Profuse itching
- Marked chemosis and injection
- Bullous chemosis may occur in severe causes or as a result of itching


Non-Infectious/Non-Allergic Conjunctivitis
- Causes
- Mechanical or chemical insult
- Patients with chronic dry eyes
- Patients s/p irrigation from chemical splash
- Transient foreign body
- Mechanical or chemical insult
- Self-limiting and spontaneously improve within 24 hours
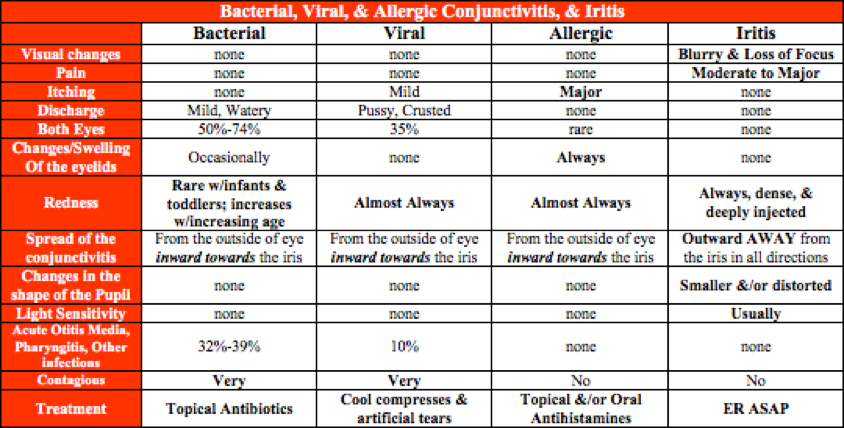
Distinguishing Between The Types

Special Considerations for Contact Lens Wearers
These patients are at an increased risk for Pseudomonas infections and should be advised to refrain from wearing their contacts and to have a formal evaluation by an ophthalmologist to rule-out serious infection. Any antibacterial treatment in these patients should also cover for Pseudomonas.
Treatment
With the exception of gonococcal conjunctivitis, all types are self-limiting and will improve on their own. Having said that, bacterial conjunctivitis will improve faster with topical antibiotics.
Bacterial
- Erythromycin 5mg/gram ointment – 1cm ribbon 4x/day for 5-7 days
- Trimethoprim-polymyxin B 0.1%-10,000 units/mL – 1-2 drops 4x/day for 5-7 days
- Ciprofloxacin 0.3% – 1-2 drops 4x/day for 5-7 days
Viral and Allergic
- Antihistamine/decongestant drops
- Pheniramine/naphazoline – 1-2 drops 4x/day
- Olopatadine 0.2% – 1 drop daily
- Azelastine 0.05% – 1 drop 2x/day
Non-Infectious/Non-Allergic
- Eye lubricants
Return to Work/School Issues
The safest recommendation is to be out until there is no longer any discharge, but this is not practical since it could last for up to 2 weeks.
Viral
- I tell patients that you treat it like the common cold and practice good hand hygiene to limit the spread of any infectious drainage
Bacterial
- Most schools require 24 hours of therapy before children are allowed to return to school
Cottage Physician

References
- Friedlaender MH. A review of the causes and treatment of bacterial and allergic conjunctivitis. Clinical therapeutics. 1995;17(5):800-10; discussion 779. [pubmed]
- Ullman S, Roussel TJ, Culbertson WW. Neisseria gonorrhoeae keratoconjunctivitis. Ophthalmology. 1987; 94(5):525-31. [pubmed]
- Wan WL, Farkas GC, May WN, Robin JB. The clinical characteristics and course of adult gonococcal conjunctivitis. American journal of ophthalmology. 1986; 102(5):575-83. [pubmed]
- Azar MJ, Dhaliwal DK, Bower KS, Kowalski RP, Gordon YJ. Possible consequences of shaking hands with your patients with epidemic keratoconjunctivitis. American journal of ophthalmology. 1996; 121(6):711-2. [pubmed]
- Roba LA, Kowalski RP, Gordon AT, Romanowski EG, Gordon YJ. Adenoviral ocular isolates demonstrate serotype-dependent differences in in vitro infectivity titers and clinical course. Cornea. 1995; 14(4):388-93. [pubmed]
- Sheikh A, Hurwitz B, van Schayck CP, McLean S, Nurmatov U. Antibiotics versus placebo for acute bacterial conjunctivitis. The Cochrane database of systematic reviews. 2012; [pubmed]
- Rose PW, Harnden A, Brueggemann AB. Chloramphenicol treatment for acute infective conjunctivitis in children in primary care: a randomised double-blind placebo-controlled trial. Lancet (London, England). ; 366(9479):37-43. [pubmed]
