
***LISTEN TO THE PODCAST HERE***
Special Guest

Janelle Bludorn, MS, PA-C is faculty at the University of North Carolina School of Medicine Physician Assistant Program as a clinical assistant professor with extensive practice history in academic emergency medicine and women’s health. She is active on social media and you can find her on Twitter @JanelleRBlu and her website http://janellebludorn.com/.
Definition of the 1st Trimester
The 1st trimester of pregnancy is from conception to week 12 gestation. It is important to note that most women do not even think about the possibility of pregnancy until 2-3 weeks post-conception and is typically after a week as passed without the initiation of a menstrual cycle. This can become even more difficult if a woman has baseline irregular menses, or the fact that early pregnancy bleeding is can occur in up to 10% of women.
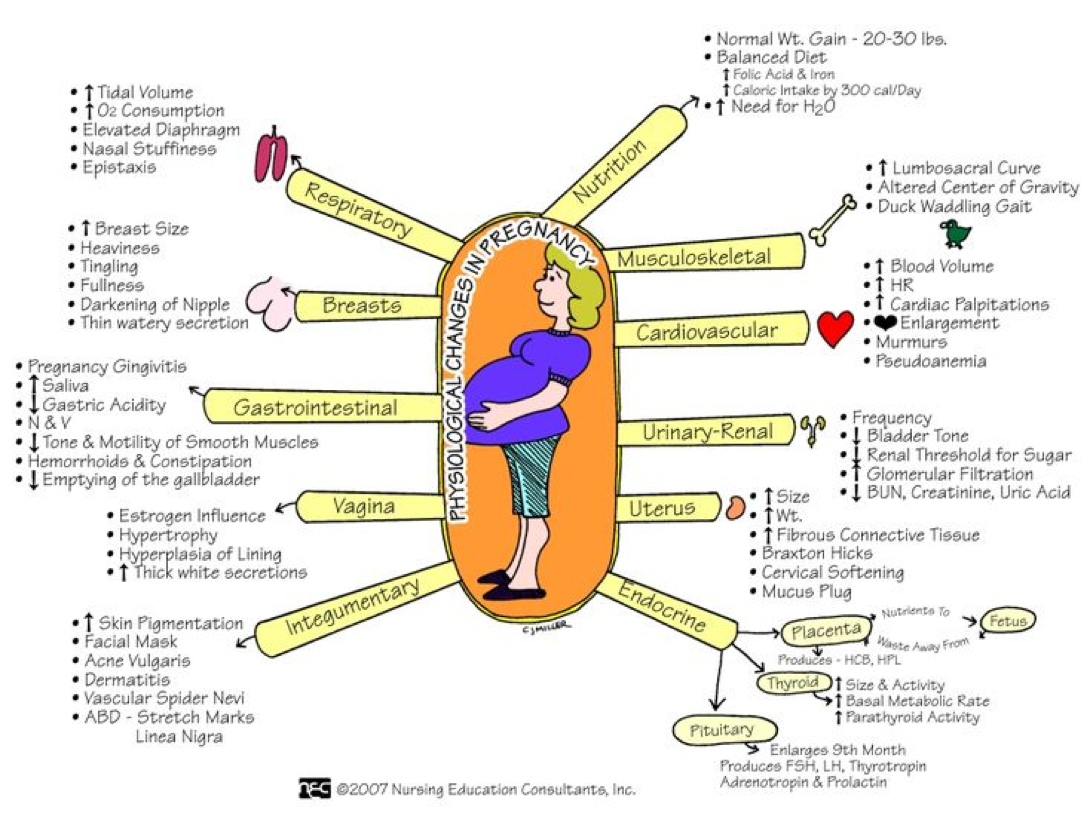
Physiological Changes of Pregnancy in 1st Trimester
- Cardiovascular
- Systemic vasodilation
- Increased plasma volume > change in RBC mass
- Increased resting heart rate
- Pulmonary
- Elevation of diaphragm
- Decreased functional residual capacity
- Increased ventilation and respiratory drive
- Gastrointestinal
- Hypomotility of bowel and gastroparesis
- Renal
- GFR increases
- BUN/Cr decreases
Signs and Symptoms of Early Pregnancy
60% of women may experience these symptoms within 6 weeks of conception and 90% will experience by 8 weeks:
- Amenorrhea
- Nausea and vomiting
- Breast enlargement and tenderness
- Increased frequency of urination without dysuria
- Fatigue
- Abdominal bloating
- Shortness of breath
- Lightheadedness
- Back pain
Physical Examination

- The uterus remains a pelvic organ until around 12 weeks gestation
- Cervix may soften (Goodell’s sign) and have a bluish color from vascular congestion (Chadwick’s sign)
- Breast become fuller, tender, and hyperpigmentation of the areola may occur
- Fetal cardiac activity can be picked up by transvaginal ultrasound as early as 6 weeks, but fetal heart tones won’t be heard until 10-12 weeks by handheld doppler
Diagnosis of Pregnancy
There are 2 ways to diagnosis pregnancy:
- Laboratory
- Detection of human chorionic gonadotropin (hCG)
- Urine (threshold – 20-50 milli-IU/mL)
- Can be detected as early as 2 weeks from fertilization
- Blood (threshold – 2-10 millil-IU/mL)
- Significantly more sensitive than urine and can be positive with a negative urine test
- Urine (threshold – 20-50 milli-IU/mL)
- Detection of human chorionic gonadotropin (hCG)
- Radiographically by ultrasound
- Gestational sac or intrauterine fluid collection may be visible at 4-5 weeks gestation
- Yolk sac appears at 5-6 weeks gestation and remains until 10 weeks
- Fetal pole with cardiac activity can be detected at 5-6 weeks (if transvaginal, closer to 6-7 weeks if transabdominal)
Errors in Laboratory Testing
- False Negatives
- Testing too soon after conception
- Hook effect
- Extremely high hCG and not diluted by lab
- False Positive
- Biochemical pregnancy
- Early fetal loss with elevated circulating hCG
- hCG from trophoblastic disease
- Biochemical pregnancy
Goals of Prenatal Care
The initial visit should occur in the 1st trimester (ideally by 10 weeks), but only 60-75% of women achieve this.
Clinical/Provider
- Early, accurate estimation of gestational age
- Identification of high risk mothers
- Ongoing evaluation of maternal and fetal health status
- Anticipatory guidance and health promotion
Mother/Patient
- Maintaining normality
- Ensuring healthy pregnancy
- Planning for effective labor and delivery
- Achieving positive motherhood transition
Components of Initial Prenatal Visit
- History
- Medical/Obstetrical
- Personal/demographic information
- Age, hospital preference, post-delivery contraception
- Past obstetrical history
- Prior pregnancies and outcomes
- Complications
- Weight and health of infants
- Any surgical obstetric history
- Family History
- History of dystocia
- History of hemorrhage
- Bleeding disorders
- Past Surgical History
- Menstrual/Gynecological history
- Recent travel
- Social History
- Tobacco, EtOH, illicit drug use
- Sexual History
- Exposure to STI
- Psychosocial
- Planned/unintended pregnancy
- Partner involvement
- Parenting plan
- Potential barriers to care
- Communication, transportation, child care, economic
- Housing
- Baseline mental health
- Screening for intimate partner violence
- Personal/demographic information
- Calculation of Gestational Age
- Naegle’s Rule
- (((1st day of the LMP) – 3 months) + 7 days) + 1 year

- MedCalc: Pregnancy Due-Dates Calculator

- Naegle’s Rule
- Physical Examination
- Physical Examination
- Blood pressure, height, and weight should be recorded
- Physical Examination
- Ultrasound Examination
- Generally not indicated unless:
- Irregular menstrual cycles
- LMP is unknown
- Conception in spite of contraception
- Uterine size discordant with menstrual dates
- ACOG recommendation – optimal timing of screening ultrasound examination is 18-22 weeks gestation.
- Generally not indicated unless:
- Aneuploidy Screening (usually between 16-20 weeks)
- ACOG recommends:
- All women be offered screening before 20 weeks gestation
- All women have the option of diagnostic invasive procedure instead of screening
- Both of these are regardless of maternal age
- 2 main categories of testing
- Maternal serum levels of biochemical markers
- Cell-free DNA in maternal circulation

- ACOG recommends:
- Laboratory Screening
- Rhesus type and antibody screen
- Rh(D)-negative women should receive prophylactic anti(D)-immune globulin at 28 weeks
- CBC
- Urine protein
- Urine culture
- Cervical cancer screening
- Infectious Disease
- HIV testing
- Documentation of rubella immunity (rubella antibody)
- Documentation of varicella immunity (varicella antibody)
- Syphilis (RPR)
- Hepatitis B (surface antigen)
- Gonorrhea and Chlamydia
- Thyroid function (TSH)
- Rhesus type and antibody screen
- Anticipatory Guidance
- Nutrition
- 300 kcal/day
- 3-6lbs in 1st trimester depending on BMI
- Exercise
- Moderate is best
- Coitus
- Safe until 1-2 weeks before delivery
- GI Complaints
- Nausea
- Small, frequent meals
- Vitamin B6 + doxylamine (Diclectin)
- GERD
- Small, frequent meals
- H2-blockers and PPI safe
- Constipation
- Stool softeners safe
- Back pain
- Stretching, acetaminophen, heating pads
- Nausea
- Nutrition
- Medical/Obstetrical



Common Complications of 1st Trimester
- Vaginal bleeding
- 20-40%
- Work-up
- Abdominal/GU physicial examination
- Serum b-hCG
- Transvaginal ultrasound{…}
- Nausea and Vomiting
- 50-75% with 1:200 women developing hyperemesis gravidarum
- Work-up
- BMP, CBC, urinalysis
- Concerned for dehydration and ketosis
- BMP, CBC, urinalysis
- Ectopic Pregnancy
- 2% of all pregnancy
- Risk Factors
- Prior tubal injury
- Tubal surgery, prior ectopic, genital tract infection
- Work-up
- Transvaginal ultrasound
- Prior tubal injury
- Gestational Trophoblastic Disease
- 4 types
- Hydatidiform mole
- Invasive mole
- Choriocarcinoma
- Placental trophoblastic tumor
- Work-up
- Serum b-hCG
- Hallmark is EXTREMELY elevated levels
- Transvaginal ultrasound
- Hallmark is “snowstorm appearance”
- Serum b-hCG
- 4 types
Time Line for Subsequent Prenatal Visits
- Every 4 weeks until 28 weeks gestation
- Every 2 weeks until 36 weeks gestation
- Every week until delivery
References
- Meah VL, Cockcroft JR, Backx K, Shave R, Stöhr EJ. Cardiac output and related haemodynamics during pregnancy: a series of meta-analyses. Heart. 2016; 102(7):518-26. [pubmed]
- Harville EW, Wilcox AJ, Baird DD, Weinberg CR. Vaginal bleeding in very early pregnancy. Human reproduction (Oxford, England). 2003; 18(9):1944-7. [pubmed]
- Foxcroft KF, Callaway LK, Byrne NM, Webster J. Development and validation of a pregnancy symptoms inventory. BMC pregnancy and childbirth. 2013; 13:3. [pubmed]
- Lohstroh P, Dong H, Chen J, Gee N, Xu X, Lasley B. Daily immunoactive and bioactive human chorionic gonadotropin profiles in periimplantation urine samples. Biology of reproduction. 2006; 75(1):24-33. [pubmed]
- Furtado LV, Lehman CM, Thompson C, Grenache DG. Should the qualitative serum pregnancy test be considered obsolete? American journal of clinical pathology. 2012; 137(2):194-202. [pubmed]
- Early Pregnancy. https://radiopaedia.org/articles/early-pregnancy
- Downe S, Finlayson K, Tunçalp Ӧ, Metin Gülmezoglu A. What matters to women: a systematic scoping review to identify the processes and outcomes of antenatal care provision that are important to healthy pregnant women. BJOG. 2016; 123(4):529-39. [pubmed]
- ACOG Committee Opinion No. 343: psychosocial risk factors: perinatal screening and intervention. Obstetrics and gynecology. 2006; 108(2):469-77. [pubmed]
- ACOG Practice Bulletin No. 88, December 2007. Invasive prenatal testing for aneuploidy. Obstetrics and gynecology. 2007; 110(6):1459-67. [pubmed]
- ACOG Practice Bulletin No. 77: screening for fetal chromosomal abnormalities. Obstetrics and gynecology. 2007; 109(1):217-27. [pubmed]
- Deutchman M, Tubay AT, Turok D. First trimester bleeding. American family physician. 2009; 79(11):985-94. [pubmed]
- Martonffy AI, Rindfleisch K, Lozeau AM, Potter B. First trimester complications. Primary care. 2012; 39(1):71-82. [pubmed]
-
Doubilet PM, Benson CB, Bourne T. Diagnostic criteria for nonviable pregnancy early in the first trimester. NEJM. 2013; 369(15):1443-51. [pubmed]
-
ACOG. Practice Bulletin No. 175: Ultrasound in Pregnancy. Obstetrics and gynecology. 2016; 128(6):e241-e256. [pubmed]
