*** LISTEN TO THE PODCAST HERE ***






Question
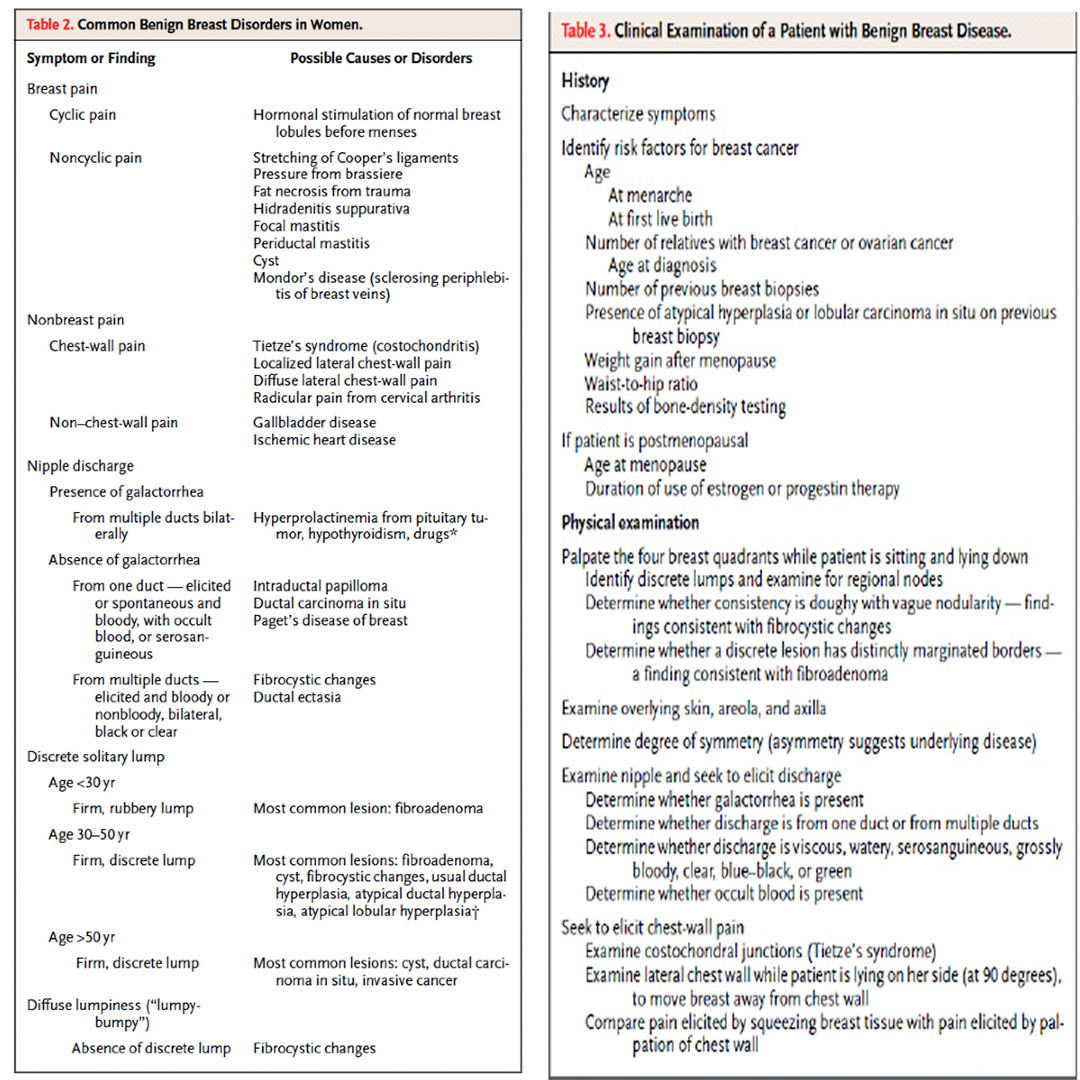
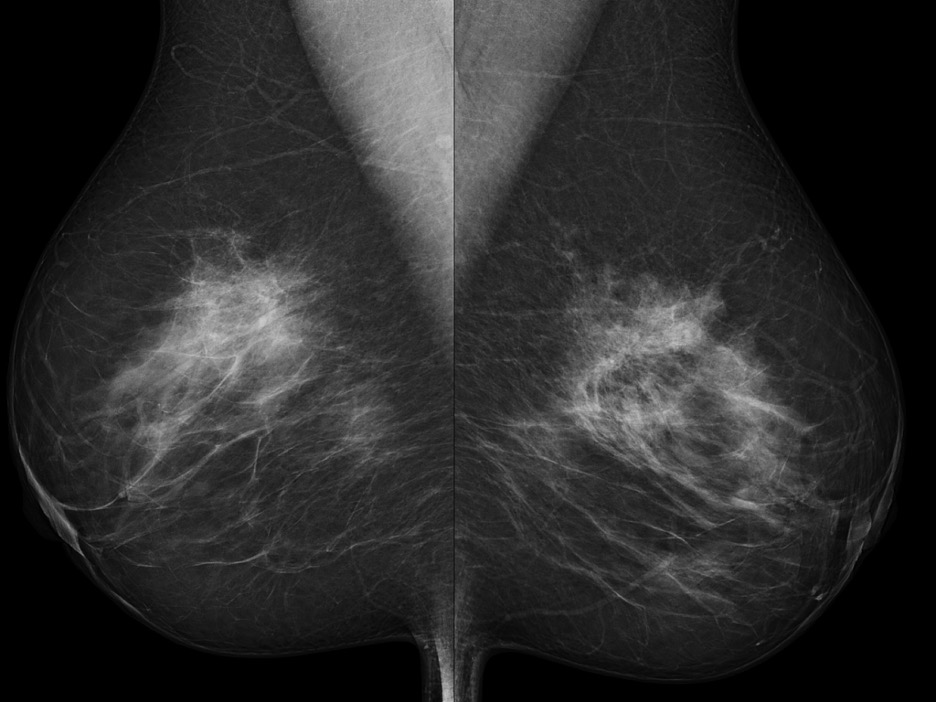
27yo, G1P1001, presents to the OBGYN office with complaints of a “breast lump”. She states she first noticed it during her pregnancy last year, but did not think anything of it until her mother told her to have it checked it out. She denies any personal or family history of malignancies or any change in size since her pregnancy. Visual inspection shows no nipple retraction, skin dimpling, or asymmetry, and physical examination reveals a 1.5cm, well-defined, non-tender mobile mass 4cm from the nipple in the 1 o’clock position.
Answer
***LISTEN TO THE PODCAST HERE***







Question
27yo, G1P1001, presents to the OBGYN office with complaints of a “breast lump”. She states she first noticed it during her pregnancy last year, but did not think anything of it until her mother told her to have it checked it out. She denies any personal or family history of malignancies or any change in size since her pregnancy. Visual inspection shows no nipple retraction, skin dimpling, or asymmetry, and physical examination reveals a 1.5cm, well-defined, non-tender mobile mass 4cm from the nipple in the 1 o’clock position.

Sampson’s Artery
Other Known Aliases – artery of the round ligament of the uterus
Definition – branch of the inferior epigastric artery that runs under and supplies the round ligament of the uterus

Clinical Significance – this artery constitutes an anastomosis of the uterine and ovarian artery and is generally considered an physiologically insignificant artery dissected during hysterectomies. However, if accidentally severed or damaged, can lead to hemoperitoneum and need for re-operation.
History – Named after John Albertson Sampson (1873-1946), an American gynecologist who received his medical doctorate from Johns Hopkins University in 1899. He would spend the majority of his career at the Albany Hospital in New York and was a pioneer in the research of endometriosis, first introducing and coining the term for this condition in 1921. He would also be the first to describe the implantation areas of endometriosis as “chocolate cysts”. It was during his time at Johns Hopkins that he took a keen interest in oncology and extensively studied the lymphatic drainage and vascular supply of the pelvis, where he was later credited with his eponymous artery of the round ligament of the uterus.

References

