
***LISTEN TO THE PODCAST HERE***
History of the Disease
The term “celiac” has Latin and Greek roots as Aretaeus of Cappadocia named this disease in the 1st century AD “koiliakos” meaning abdomen/abdominal in patients with chronic diarrhea. The first modern medical description of the disease was in 1888 by Samuel Gee in an paper entitled “On the Coeliac Affection”. The specific medical term for Celiac Disease is “gluten-sensitive enteropathy”. It was still relatively unexplained until Willem Dicke, a Dutch pediatrician, noted improvement in his patient’s abdominal symptoms during bread and grain shortages of World War II.
Epidemiology
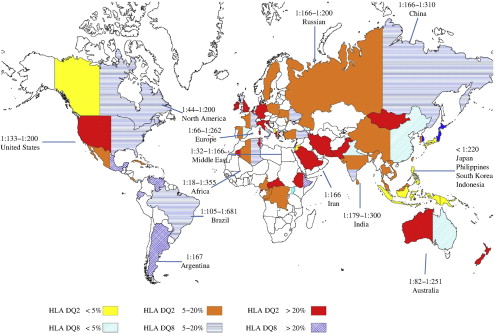
- Primarily in northern European white
- Prevalence is widely variable due to differing rates and types of population screening throughout the world

Pathophysiology
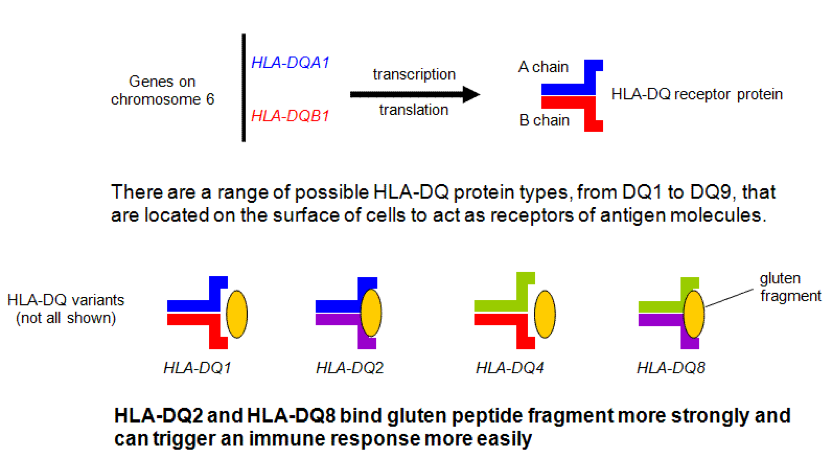
High association with genetic predisposition to gluten sensitivity, specifically HLA-DQ2 and/or DQ8, and because of these genetic changes, serum autoantibodies are produced that attack the endomysium of the enterocytes of the small bowel.
Signs and Symptoms
Originally thought to be a disease of infancy, it is being diagnosed later and later in life, with adults first being diagnosed as late as the fifth decade. Often, this is in the setting of failure to thrive in an infant.
Common
- Diarrhea
- Steatorrhea
- Malabsorption
- Anemia (iron), weight loss,
metabolic bone disease (vitamin D and calcium), vitamin deficiencies (B-complex
vitamins)
- Peripheral neuropathy, ataxia
- Anemia (iron), weight loss,
metabolic bone disease (vitamin D and calcium), vitamin deficiencies (B-complex
vitamins)
Associated Clinical Findings
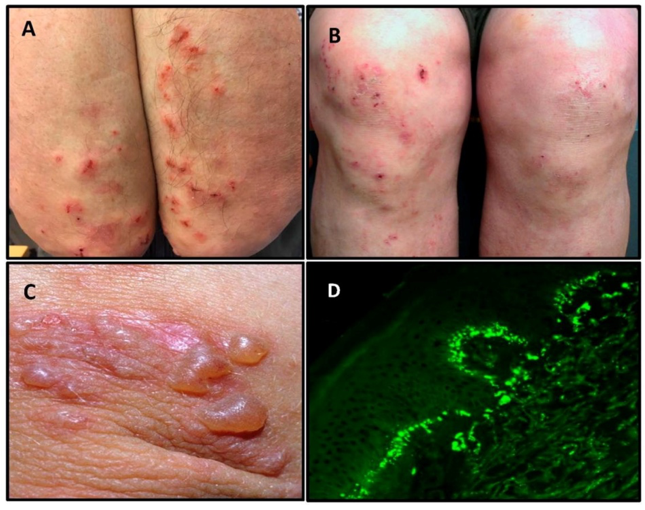
- Dermatitis herpetifomis
- Pruritic papules and grouped vesicles on the elbows, forearms, knees, scalp, back, and buttock.
- 1:369 patients diagnosed with celiac disease
- Diagnosed with biopsy histologic evidence of IgA deposition in basement membrane
- Down Syndrome
- As high as 16% association, which isa 20-fold increase compared with general public
- Also associated with liver disease, diabetes, thyroid disease, inflammatory bowel disease
Screening and Diagnosis
- Who should be screened?
- Patients with chronic diarrhea, malabsorption, weight loss, or abdominal distension and bloating
- Patients without other explanations for extraintestinal diseases such as anemia, elevated transaminases, peripheral neuropathy, ataxia, etc.
- Patients with type 1 DM and signs or symptoms of celiac disease
- Asymptomatic first-degree relatives of patients with confirmed celiac disease
- Immunoglobulin A (IgA) anti-tissue
transglutaminase (TTG) is the initial screening test of choice
- If positive, then proceed with duodenal biopsy via endoscopy
- If negative, HLA-DQ2/DQ8 testing is
performed to evaluate for nonceliac gluten sensitivity
- If negative, then celiac is ruled-out
- If positive, then slow introduction
of gluten-containing foods is started
- If unable to tolerate, then proceed with biopsy
- If serology changes to positive, then celiac disease is confirmed

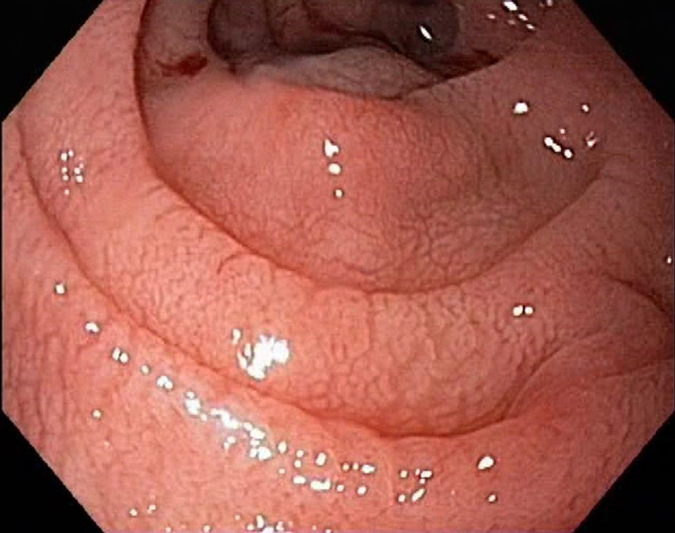
- Endoscopic biopsy is the confirmatory
test of choice in patients with positive serologic screening and high
probability of celiac disease.
- Duodenal mucosa may appear atrophic with loss of folds, visible fissures, nodular folds, and/or scalloped appearance
- Histologic features of small bowel biopsy include increased intraepithelial lymphocytes, flat mucosa with complete loss of villi and atrophy, and/or crypt hyperplasia

Classification
Celiac disease can present as a spectrum of signs and symptoms and thus, have different classifications.
- Classic Disease
- 3 key features
- Villous atrophy
- Symptoms of malabsorption
- Steatorrhea, weight loss, nutrient deficiencies
- Improvement in symptoms with withdrawal of gluten-containing foods
- 3 key features
- Atypical Disease
- Minor gastrointestinal complaints
- Anemia, osteoporosis, tooth enamel issues,
- Severe mucosal damage is present on endoscopy
- Asymptomatic (Silent) Disease
- Incidental finding on screening without symptoms
Management
Six key elements of successful management of celiac disease and it has a nice acronym:
- Consultation with a skilled dietician
- Education about the disease
- Lifelong adherence to a gluten-free diet
- Identification and treatment of nutritional deficiencies
- Access to an advocacy group
- Continuous long-term follow-up by a multidisciplinary team
Cottage Physician
This is an excerpt from the pediatric disease section on diarrhea:
References
- Impact – A Publication of the University of Chicago Celiac Disease Center. 2007;7(3):1-3. [article]
- Yan D, Holt PR. Willem Dicke. Brilliant clinical observer and translational investigator. Discoverer of the toxic cause ofceliac disease. Clinical and translational science. 2009; 2(6):446-8. [pubmed]
- Schuppan D. Current concepts of celiac disease pathogenesis. Gastroenterology. 2000; 119(1):234-42. [pubmed]
- Kagnoff MF. Celiac disease. A gastrointestinal disease with environmental, genetic, and immunologic components.Gastroenterology clinics of North America. 1992; 21(2):405-25. [pubmed]
- Dieterich W, Laag E, Schöpper H, et al.Autoantibodies to tissue transglutaminase as predictors of celiac disease.Gastroenterology. 1998; 115(6):1317-21. [pubmed]
- Sulkanen S, Halttunen T, Laurila K, et al.Tissue transglutaminase autoantibody enzyme-linked immunosorbent assay in detecting celiac disease. Gastroenterology. 1998; 115(6):1322-8. [pubmed]
- Fasano A, Catassi C. Clinical practice. Celiacdisease. The New England journal of medicine. 2012; 367(25):2419-26. [pubmed]
- Leonard MM, Sapone A, Catassi C, Fasano A.Celiac Disease and Nonceliac Gluten Sensitivity: A Review. JAMA. 2017;318(7):647-656. [pubmed]
- Guandalini S, Assiri A. Celiac disease: areview. JAMA pediatrics. 2014; 168(3):272-8. [pubmed]
- Bibbins-DomingoK, Grossman DC, et al. Screening for Celiac Disease: US Preventive Services Task Force Recommendation Statement. JAMA. 2017; 317(12):1252-1257. [pubmed]
- CarlssonA, Axelsson I, Borulf S, et al. Prevalence of IgA-antigliadin antibodies and IgA-antiendomysium antibodies related to celiac disease in children with Down syndrome. Pediatrics. 1998; 101(2):272-5. [pubmed]
- Rubio-TapiaA, Hill ID, Kelly CP, Calderwood AH, Murray JA, . ACG clinical guidelines:diagnosis and management of celiac disease. The American journal of gastroenterology. 2013; 108(5):656-76; quiz 677. [pubmed]
- ShahVH, Rotterdam H, Kotler DP, Fasano A, Green PH. All that scallops is not celiac disease. Gastrointestinal endoscopy. 2000; 51(6):717-20. [pubmed]
- OberhuberG, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for astandardized report scheme for pathologists. European journal of gastroenterology & hepatology. 1999; 11(10):1185-94. [pubmed]
- National Institutes of Health Consensus Development Conference Statement on Celiac Disease, June 28-30, 2004.Gastroenterology. 2005; 128(4 Suppl 1):S1-9. [pubmed]
