

***LISTEN TO THE PODCAST HERE***
Definitions
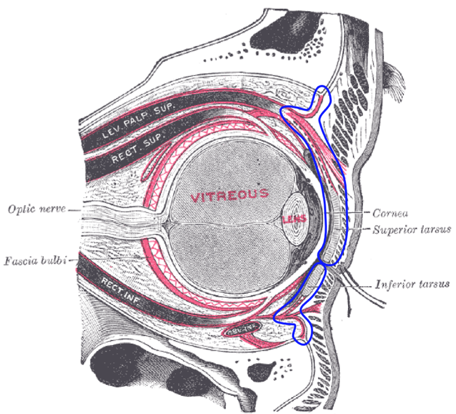
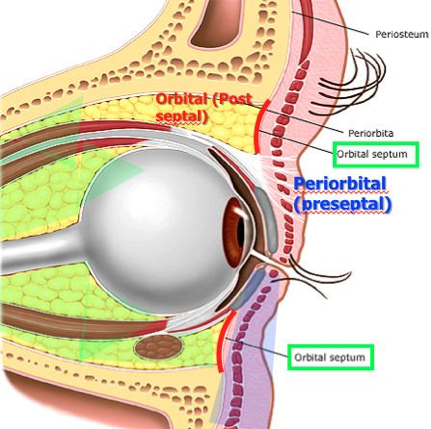
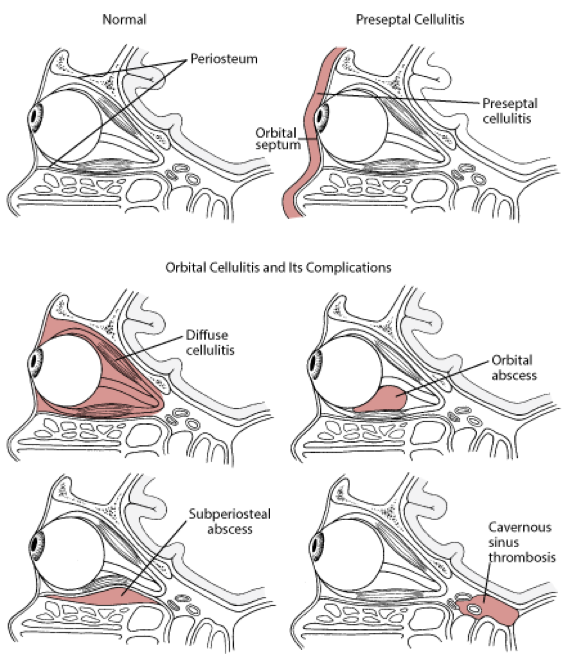
- Orbital Septum
- Membranous structure that extends from orbit to the tarsal plate and is the anterior boundary of the orbital compartment
- Preseptal Cellulitis
- Infection of the soft tissues ANTERIOR to the orbital septum
- Orbital Cellulitis
- Infections of the soft tissues POSTERIOR to the orbital septum
Numbers
- Preseptal cellulitis is much more common than orbital (>90%)
- Both conditions are more common in children than adults
Pathogenesis
- Preseptal
- Usually due to superficial dermatologic infections (though the data has wide variability in reported causes)
- Orbital
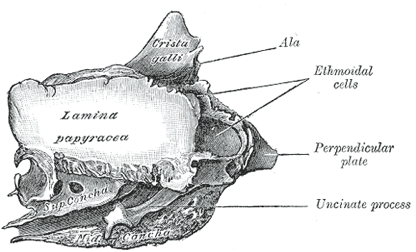
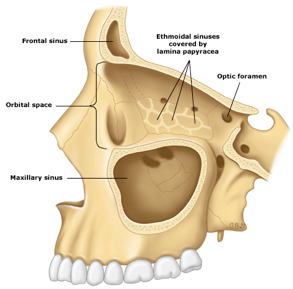
- Bacterial rhinosinusitis
- Due to perforations in the lamina papyracea
- Other causes:
- Ophthalmologic surgery
- Dacrocystitis
- Orbital trauma
- Dental infections
- Bacterial rhinosinusitis
Microbiology
- Preseptal
- Staphylococcus aureus (skin causes)
- Increasing incidence of MRSA
- Streptococcus pneumoniae (sinus/nasopharynx causes)
- Staphylococcus aureus (skin causes)
- Orbital
- Same as preseptal, but include:
- Fungal (mucormycosis and Aspergillus spp.)
- Same as preseptal, but include:
Signs and Symptoms
- Both present with unilateral eyepain, erythema, and edema, but:
- Preseptal
- No pain with eye movement
- Sclera is white

- Orbital
- Painful eye movement
- Vision changes (acuity, diplopia)
- Proptosis
- Sclera injection and chemosis
- Decreased pupillary response
- Orbital

Complications
- Complications of preseptal cellulitis are rare, but orbital cellulitis can lead to:
- Vision loss (3-11%)
- Subperiosteal abscess
- Orbital abscess
- Cavernous sinus thrombosis
Diagnostic Studies
- CBC with differential may be helpful in risk stratification or atypical presentation
- Preseptal
- None! –> Clinical diagnosis
- Orbital
- Indications for CT scan
- Inability to assess vision or deteriorating vision
- Double vision
- Inability to examine due to age
- Proptosis
- Restricted, limited, and/or painfuleye movement
- Edema extending beyond eyelid margin
- Lack of improvement in 24 hours on antibiotics
- Cyclical fevers
- Signs of CNS involvement
- ANC > 10,000 cell/microL
- Indications for CT scan


- Blood cultures are not routinely recommended but should be entertained in ill appearing children prior to antibiotic administration
Treatment
- Preseptal
- Outpatient
- > 1 year old and no signs of systemic toxicity
- Treatment duration typically 5-7days, but treatment should continue until eyelid erythema and swelling have resolved
- Inpatient
- < 1 year old, children who can’t cooperate with exam, toxic appearance, or outpatient treatment failing to improve in 24-48 hours
- Follow orbital cellulitis treatment
- Outpatient

- Orbital
- Medical
- Staphylococcal coverage
- Vancomycin
- Streptococcal coverage
- Ceftriaxone
- Cefotaxime
- Anaerobic coverage
- Metronidazole
- Improvement should occur within24-48 hours
- Transition to oral therapy when:
- Afebrile and periorbital signs are resolving
- Typically 3-5 days
- Follow culture data (if obtained) or follow outpatient preseptal cellulitis regimen
- Treat for a total of 2-3 weeks
- Staphylococcal coverage
- Surgical indications
- Radiographically identified abscess
- Typically > 10mm, though small abscesses respond to antibiotics well
- Intracranial extension
- Failure to respond to antibiotic treatment
- Threat to vision
- Radiographically identified abscess
- Medical
References
- Hauser A, Fogarasi S. Periorbital and orbital cellulitis. Pediatrics in review. 2010; 31(6):242-9. [pubmed]
- Botting AM, McIntosh D, Mahadevan M. Paediatric pre- and post-septal peri-orbital infections are different diseases. A retrospective review of 262 cases. International journal of pediatric otorhinolaryngology. 2008; 72(3):377-83. [pubmed]
- Horton JC. Disorders of the Eye. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e New York, NY: McGraw-Hill; http://accessmedicine.mhmedical.com/content.aspx?bookid=2129§ionid=192011900
- Chaudhry IA, Shamsi FA, Elzaridi E, Al-Rashed W, Al-Amri A, Arat YO. Inpatient preseptal cellulitis: experience from a tertiary eye care centre. The British journal of ophthalmology. 2008; 92(10):1337-41. [pubmed]
- Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. The New England journal of medicine. 2006; 355(7):666-74. [pubmed]
- Brook I, Frazier EH. Microbiology of subperiosteal orbital abscess and associated maxillary sinusitis. The Laryngoscope. 1996; 106(8):1010-3. [pubmed]
- Erickson BP, Lee WW. Orbital Cellulitis and Subperiosteal Abscess: A 5-year Outcomes Analysis. Orbit (Amsterdam, Netherlands). 2015; 34(3):115-20. [pubmed]
- Howe L, Jones NS. Guidelines for the management of periorbital cellulitis/abscess. Clinical otolaryngology and allied sciences. 2004; 29(6):725-8. [pubmed]
- Rudloe TF, Harper MB, Prabhu SP, Rahbar R, Vanderveen D, Kimia AA. Acute periorbital infections: who needs emergent imaging? Pediatrics. 2010; 125(4):e719-26. [pubmed]
- Tanna N, Preciado DA, Clary MS, Choi SS. Surgical treatment of subperiosteal orbital abscess. Archives of otolaryngology–head & neck surgery. 2008; 134(7):764-7. [pubmed]
- Greenberg MF, Pollard ZF. Medical treatment of pediatric subperiosteal orbital abscess secondary to sinusitis. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 1998; 2(6):351-5. [pubmed]
