
***LISTEN TO THE PODCAST HERE***
Definition
- Group of disorders that cause a
metabolic acidosis due to defects in the renal tubules
- Net retention of HCl
- Net loss of NaHCO3
Pathophysiology
The kidney regulates acid-base balance two main ways:
- Reabsorption of filtered HCO3
- >80% of the bicarbonate filtered by the glomerulus is reabsorbed in the proximal renal tubules via Na-H exchange


- Acid excretion
- Collecting ducts of the nephron excrete hydrogen ions buffered by NH3 and PO3 (so the pH of the urine doesn’t destroy the nephron)
- Extra production of NH3 is stimulated by intracellular acidosis.
- Collecting ducts of the nephron excrete hydrogen ions buffered by NH3 and PO3 (so the pH of the urine doesn’t destroy the nephron)


- 3 step process
- Reabsorption of sodium to create a negative gradient in the tubular lumen
- Excretion of hydrogen by H-K-ATPase and reabsorption of potassium
- Prevention of hydrogen ions from diffusing back out of the tubular lumen
Initial Presentation
- Patients diagnosed with an RTA must first be diagnosed with a metabolic acidosis
- Decreased pH with decreased HCO3
- After this is determined, the anion gap must be calculated and found to be normal
- AG = Na – (Cl + HCO3) = 8-12
Differential for NAGMA
- Ureteric diversion
- Small bowel fistulae
- Excessive saline
- Diarrhea
- Carbonic anhydrase inhibitors
- Renal tubular acidosis
- Adrenal insufficiency
- Pancreatic fistulae
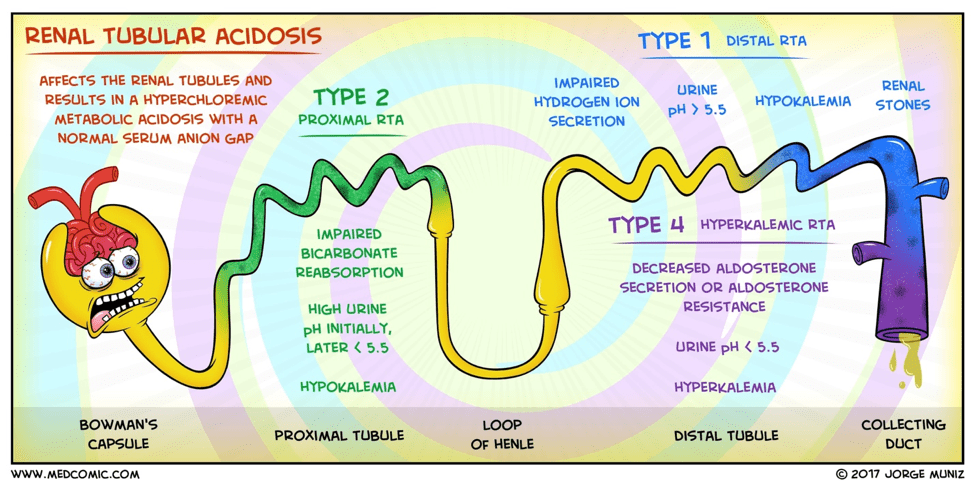
Type I (distal) RTA
- Cause
- Defect in the distal hydrogen ion excretion
- Pathophysiology
- Failure of the H-ATPase proton pump
(most common cause)
- Inability to acidify urine < 5.5
- Hypokalemia
- Increased hydrogen ion permeability of the luminal membrane
- Failure of the H-ATPase proton pump
(most common cause)

Type II (proximal) RTA
- Cause
- Defect in proximal bicarbonate reabsorption
- Pathophysiology
- Damage to the proximal tubule that leads to progressive bicarbonate wasting in the urine

Type IV (hypoaldosteronism)
- Cause
- Reductions in aldosterone secretion and responsiveness
- Pathophysiology
- Decreased rate of proton secretion rather than an intrinsic defect in the tubule’s capacity to generate normal pH gradient
- Hyperkalemia causes reduced urine
NH4, which in turns leads to more acidic urine
- Hydrogen ions have nothing to bind to
Diagnostic Work-Up
- RTAs should be considered in any
patient with a normal anion gap metabolic acidosis
- Need ABG and BMP
- Once this determination is made:
- Urine pH
- > 5.5 in type I (distal)
- < 5.5 in type II (proximal) and type IV
- Urine ammonium
- Elevated in type II (proximal)
- Decreased in type I (distal) and type IV
- Most labs can’t measure urine
ammonium directly:
- Urine Anion Gap (urine Na+K+Cl)
- (+) UAG = > 20
- Type I (distal) and type IV
- (-) UAG = < – 20
- Type II (proximal)
- (+) UAG = > 20
- Urine Anion Gap (urine Na+K+Cl)
- Serum potassium
- Elevated in type IV
- Decreased in type I and II
- Urine pH

Treatment
- Type I (distal)
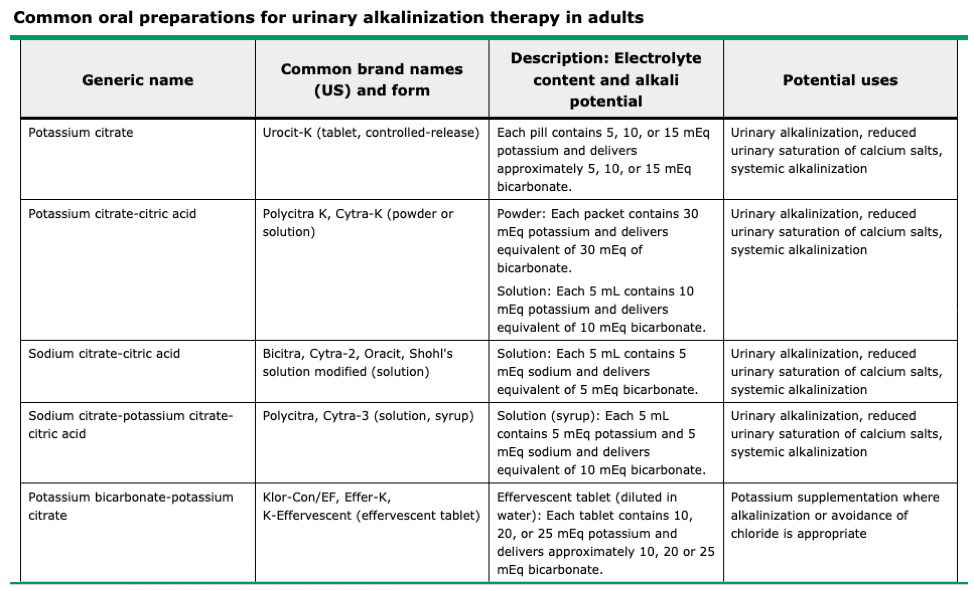
- Urinarary Alkali Therapy
- Sodium bicarbonate
- Increased risk of nephrolithiasis due
to bicarbonaturia
- Use potassium citrate instead
- Increased risk of nephrolithiasis due
to bicarbonaturia
- Sodium bicarbonate
- Urinarary Alkali Therapy
- Type II (proximal)
- Much more difficult to treat due to the INCREASED bicarbonate diuresis during bicarbonate therapy
- Alkali therapy (10x the dose for type I) AND potassium salt repletion as bicarbonaturia INCREASES urinary potassium losses
- Thiazide diuretics if large alkali
doses ineffective or not tolerated
- Diuresis reduces urinary bicarbonate
loss by increasing proximal sodium reabsorption
- Which secondarily increased bicarbonate reabsorption
- Diuresis reduces urinary bicarbonate
loss by increasing proximal sodium reabsorption
- Type IV
- Stop any medication causes or treat
underlying condition (hypoaldosteronism)
- Mineralcorticoid (fludrocortisone) and glucocorticoid (hydrocortisone)
- Potassium repletion
- Stop any medication causes or treat
underlying condition (hypoaldosteronism)
References
- Rodríguez Soriano J. Renal tubular acidosis: the clinical entity. Journal of the American Society of Nephrology : JASN. 2002; 13(8):2160-70. [pubmed]
- Skelton LA, Boron WF, Zhou Y. Acid-base transport by the renal proximal tubule. Journal of nephrology. ; 23 Suppl 16:S4-18. [pubmed]
- Hamm LL, Nakhoul N, Hering-Smith KS. Acid-Base Homeostasis. Clinical journal of the American Society of Nephrology : CJASN. 2015; 10(12):2232-42. [pubmed]
- The Curbsiders. Episode 104. https://thecurbsiders.com/internal-medicine-podcast/104-renal-tubular-acidosis-kidney-boy-joel-topf-md
- DB’s Medical Rants. http://www.medrants.com/archives/8897
- Oh M, Carroll HJ. Value and determinants of urine anion gap. Nephron. 2002; 90(3):252-5. [pubmed]
- Rodríguez Soriano J. Renal tubular acidosis: the clinical entity. Journal of the American Society of Nephrology : JASN. 2002; 13(8):2160-70. [pubmed]
- Karet FE. Mechanisms in hyperkalemic renal tubular acidosis. Journal of the American Society of Nephrology : JASN. 2009; 20(2):251-4. [pubmed]
