*** LISTEN TO THE PODCAST HERE ***




***LISTEN TO THE PODCAST HERE***

***LISTEN TO THE PODCAST HERE***

***LISTEN TO THE PODCAST HERE***

***LISTEN TO THE PODCAST HERE***














Question
Surgery is a major physiologic stress and often is accompanied by biochemical derangements that effect homeostasis in the post-operative period. Describe the most common clinical scenarios that can cause each of the four main acid-base imbalances in a post-surgical patient.
Answer

Question
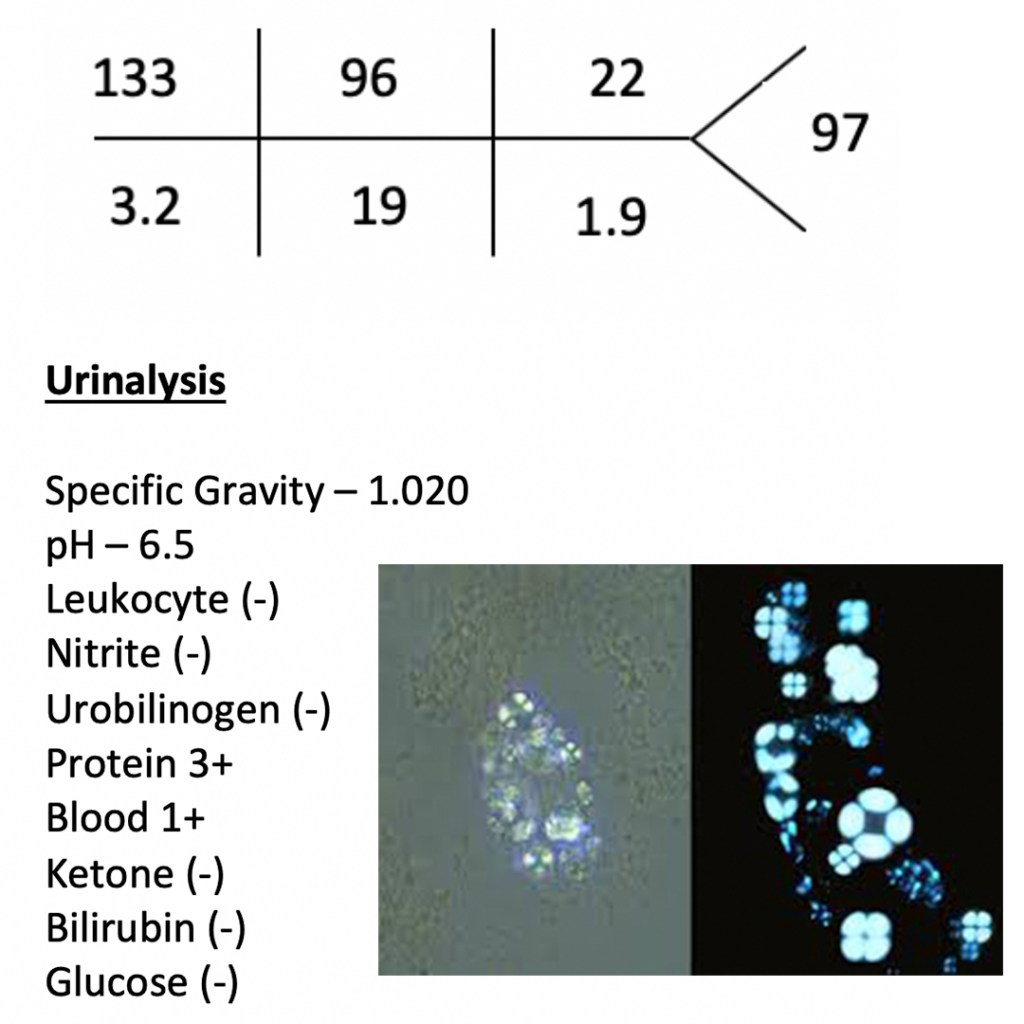
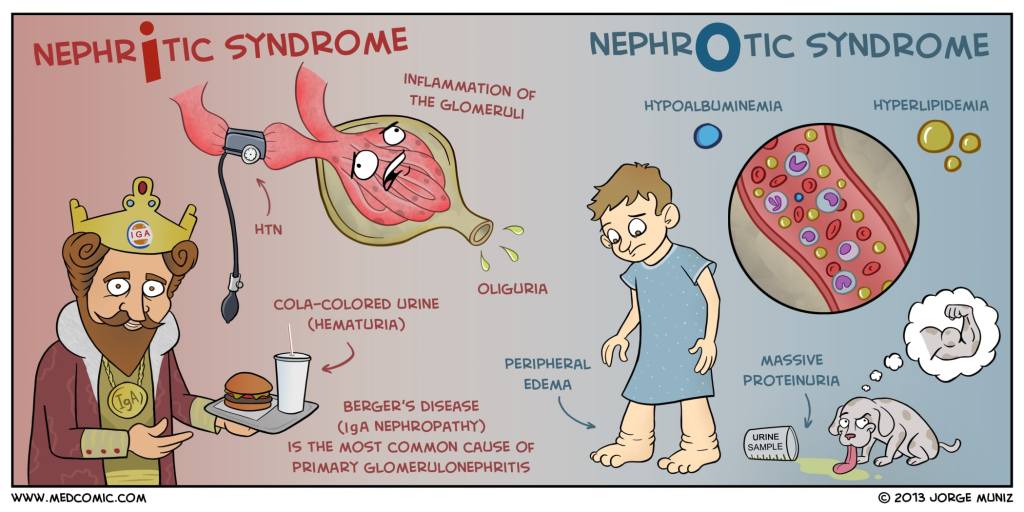
42yo woman, with a history systemic lupus erythematosus, presents to your clinic with a 1-month history of progressive leg swelling and polyuria. She is complaint with her medications and states that she hasn’t changed anything in her medical care. Physical examination reveals 2+ pitting edema to the knees in the lower extremities. BMP, UA, and urine microscopy are below.
Answer
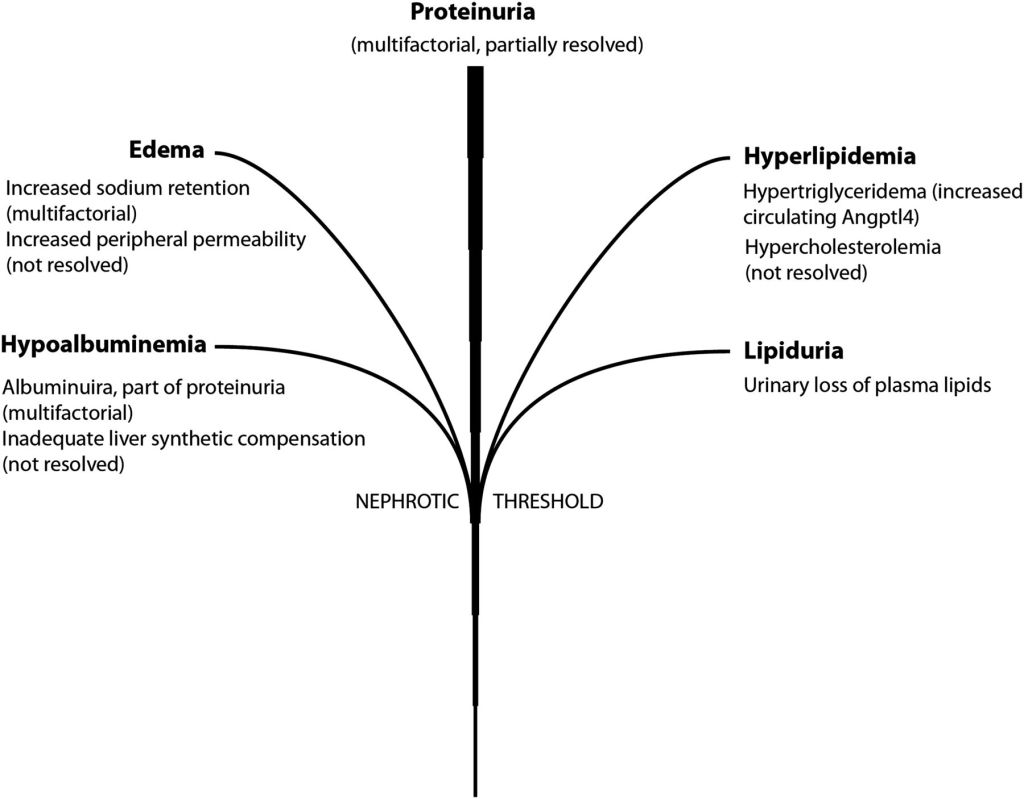
This patient found to heavy proteinuria on a urinalysis and oval fat bodies on urine microscopy, which would point to nephrotic syndrome as a diagnosis.
The next step in the diagnostic management of this patient would be to perform a 24-hour urine collection for urine protein. Normal urine protein excretion is < 150mg/day, but nephrotic range proteinuria is diagnostic at > 3.5g/day. Alternatively, a random urine protein-to-creatinine ratio of > 3.5 can be used, but is less reliable than a 24-hour collection.
Once a nephrotic syndrome diagnosis is made by urine studies, it should be followed up with a renal biopsy to determine the cause.
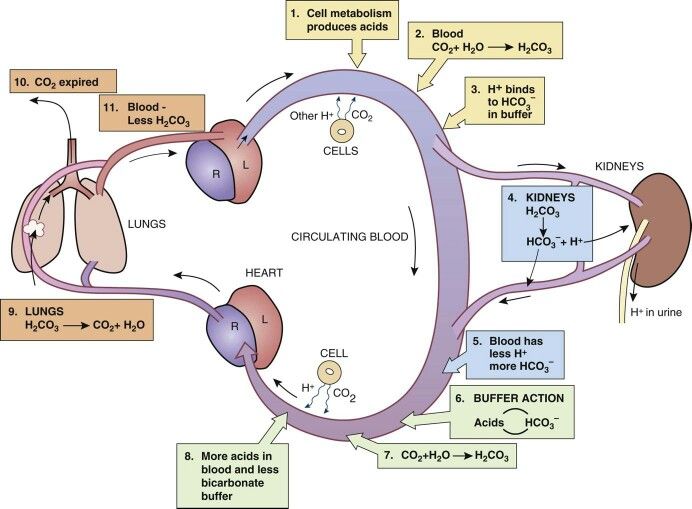
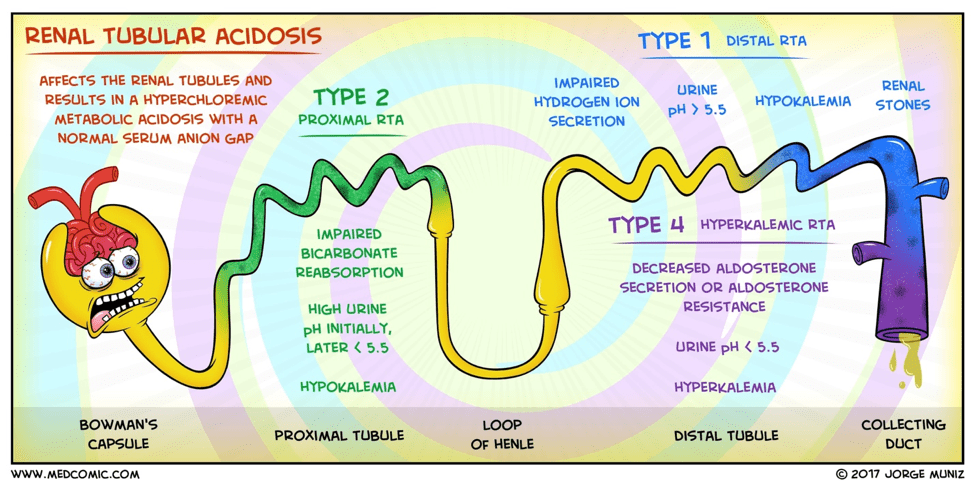
The kidney regulates acid-base balance two main ways:








Question
42yo woman, with a history systemic lupus erythematosus, presents to your clinic with a 1-month history of progressive leg swelling and polyuria. She is complaint with her medications and states that she hasn’t changed anything in her medical care. Physical examination reveals 2+ pitting edema to the knees in the lower extremities. BMP, UA, and urine microscopy are below.

