

***LISTEN TO THE PODCAST HERE***
Definition
- Infection of the lacrimal sac usually due to obstruction of the nasolacrimal systems
Anatomy
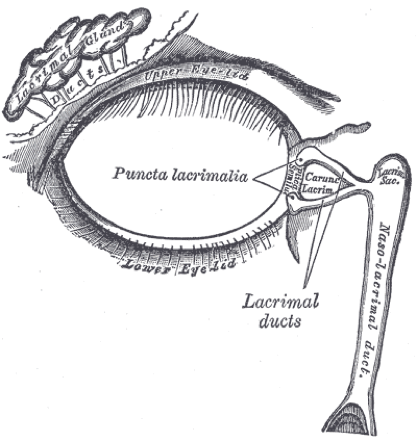
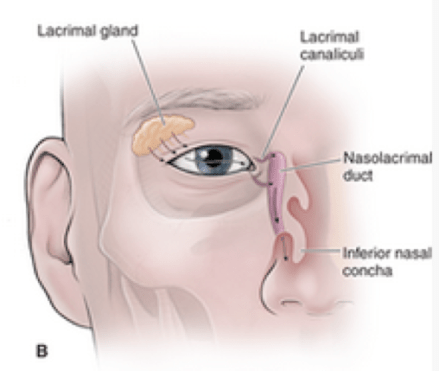
The lacrimal apparatus is responsible for tear production and drainage of the eye and consists of 3 main structures:
- Lacrimal gland
- Serous gland located in the superiorlateral corner of the orbit in the lacrimal fossa
- Responsible for tear secretion onto the globe
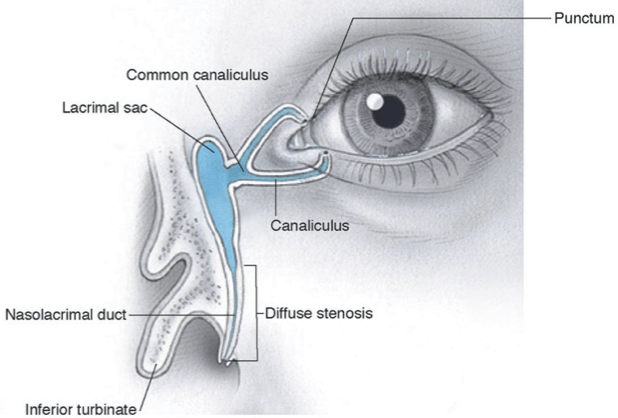
- Lacrimal canaliculi
- Drainage ducts located in the medial corner of the eye and drain into the nasolacrimal duct
- Nasolacrimal duct
- Drains into the inferior nasal meatus of the nasal cavity
Pathophysiology
- The most common cause of dacryocystitis is obstruction of the nasolacrimal duct
- Adults
- Chronic inflammation leading to fibrosis/stenosis of the duct
- Most commonly in postmenopausal women
- Infants/Children
- Persistent membrane covering the Valve of Hasner
- Occurs in up to 90% of newborns
- Becomes patent by the end of the first month of life in 90%
- Occurs in up to 90% of newborns
- Persistent membrane covering the Valve of Hasner

Microbiology
- Pediatric
- Streptococcus pneumoniae
- Staphylococcus species
- Haemophilus influenza
- Entrobacteriaceae species
- Adults
- Staphylococcus aureus
- Staphylococcus epidermidius
- Pseudomonas aeruginosa
- Propionibacterium species
Clinical Findings
- The main clinical finding is tearing and discharge
- Acute
- Inflammation, pain, swelling, and tenderness beneath the medial canthal tendon around the lacrimal sac
- Purulence can be expressed through the lacrimal puncta with direct pressure on the lacrimal sac
- Inflammation, pain, swelling, and tenderness beneath the medial canthal tendon around the lacrimal sac


- Chronic
- Tearing and matting of the eyelashes is most common
- Mucoid material can be expressed occasionally

Diagnostic Studies
- Although this is clearly a clinical diagnosis and the majority do not need further studies, you can do a bedside test called “Dye Disappearance Test”
- Apply a drop of topical anesthetic
- Place a drop of fluorescein stained saline in the inferior cul-de-sac of each of the patient’s eyes
- Wipe away excess tears from eyelids
- Observe patient for 5 minutes with careful instructions that the eye should not be rubbed and cheeks should not be wiped
- After 5 minutes inspect eye, nose, and cheek
- All of the fluorescein should have drained into the nose within 5 minutes if there is no obstruction
- If any fluorescein remains in eye or drained down the cheek, then the test is positive

Treatment
- Most cases respond to appropriate systemic antibiotic therapy
- Culture expressed purulence to aid in antibiotic selection
- Acute (7-10 days of therapy)
- Mild cases – Clindamycin
- Severe – Vancomycin + 3rd generation cephalosporin
- For infants:
- External digital massage of the lacrimal sac is first line
- Increases the hydrostatic pressure to force open the obstructed membrane
- External digital massage of the lacrimal sac is first line

- Nasolacrimal probing is indicated in acute cases and cases persisting for > 6 months
- Some cases require balloon dilation, silicone stent placement, or inferior turbinate fracture
- For adults:
- Chronic topical antibiotic drops can help keep patent, but this is only symptomatic relief
- Fluoroquinolones – moxifloxacin, ciprofloxacin, ofloxacin
- Aminoglycoside – tobramycin, gentamicin
- Dacryocystorhinostomy is required to prevent recurrence
- Permanent fistula formed between lacrimal sac and the nose
- Chronic topical antibiotic drops can help keep patent, but this is only symptomatic relief
The Cottage Physician (1893)


References
- Duncan JL, Parikh NB, Seitzman GD, Riordan-Eva P. Disorders of the Lids & Lacrimal Apparatus. In: Papadakis MA, McPhee SJ, Rabow MW. eds. Current Medical Diagnosis and Treatment 2020. New York, NY: McGraw-Hill
- Orbit. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy, 2e New York, NY: McGraw-Hill;
- Vagefi M. Lids & Lacrimal Apparatus. In: Riordan-Eva P, Augsburger JJ. eds. Vaughan & Asbury’s General Ophthalmology, 19e New York, NY: McGraw-Hill
- Horton JC. Disorders of the Eye. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e New York, NY: McGraw-Hill
- Hoffmann J, Lipsett S. Acute Dacryocystitis. The New England journal of medicine. 2018; 379(5):474. [pubmed]
- Campolattaro BN, Lueder GT, Tychsen L. Spectrum of pediatric dacryocystitis: medical and surgical management of 54 cases. Journal of pediatric ophthalmology and strabismus. ; 34(3):143-53; quiz 186-7. [pubmed]
- Qian Y, Traboulsi EI. Lacrimal sac compression, not massage. Journal of pediatric ophthalmology and strabismus. ; 46(4):252. [pubmed]
- Örge FH, Boente CS. The lacrimal system. Pediatric clinics of North America. 2014; 61(3):529-39. [pubmed]
