

***LISTEN TO THE PODCAST HERE***
Definitions
- 1980 – WHO characterized cardiomyopathies as “heart muscle diseases of unknown causes”
- Distinguish between non-cardiovascular pathologies (HTN, coronary disease, valvular disease)
- 1995 – WHO and International Society and Federation of Cardiology (ISFC) developed a task force specifically looking at the definition and classifications of cardiomyopathies
- Definition they developed was “disease of the myocardium associated with cardiac dysfunction”
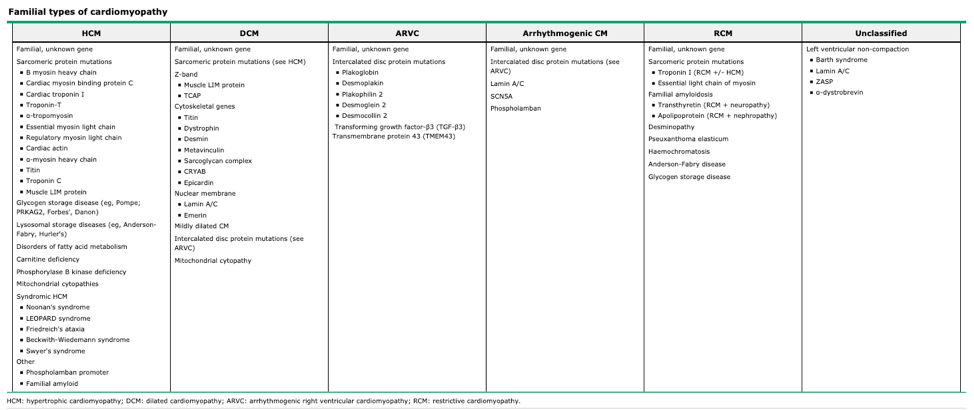
- Dilated cardiomyopathy (DCM)
- Hypertrophic cardiomyopathy (HCM)
- Restrictive cardiomyopathy (FCM)
- Arrhythmogenic right ventricular cardiomyopathy (ARVC)
- Unclassified cardiomyopathy
- Definition they developed was “disease of the myocardium associated with cardiac dysfunction”
- 2006 – AHA released a statement to update to a more contemporary definition with two major categories
- Primary cardiomyopathies (predominantly involving the heart)
- Genetic
- HCM, ARVC
- Mixed
- DCM, RCM
- Acquired
- Myocarditis, stress-induced, peripartum, tachy-induced
- Genetic
- Secondary cardiomyopathies (other system involvement)
- Primary cardiomyopathies (predominantly involving the heart)
- 2008 – European Society of Cardiology (ESC) updated the WHO/IFSC classification of cardiomyopathies as
- “a disorder in which the heart muscle is structurally and functionally abnormal in the absence of coronary artery disease, HTN, valvular disease, and congenital heart disease”
- Meant to more clinically useful
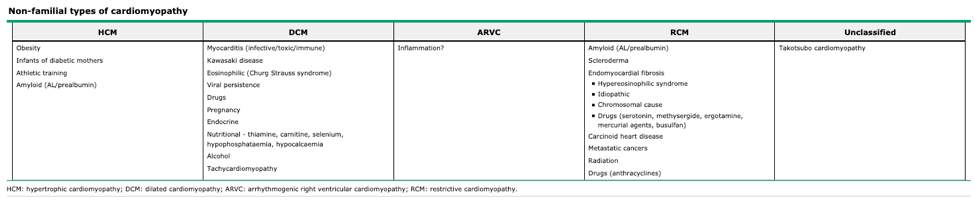
- Further subcategorized into familial and non-familial causes, as well as removing CAD, vavlvular, congenital heart disease, and ion channelopathies as causes
- “a disorder in which the heart muscle is structurally and functionally abnormal in the absence of coronary artery disease, HTN, valvular disease, and congenital heart disease”
Echographic Evaluation
- Systolic
- Decrease in myocardial contractility resulting in a decrease in left ventricular ejection fraction
- To compensate, cardiac output is maintained by LV enlargement (increase stroke volume)
- As a result, systolic dysfunction is most commonly characterized by a dilated cardiomyopathy
- Decrease in myocardial contractility resulting in a decrease in left ventricular ejection fraction
- Diastolic
- Dysfunction in LV relaxation resulting in abnormal filling and elevated filling pressures
- Mostly affected by compliance and distensibility of the myocardium
- As a result, diastolic dysfunction is most commonly characterized by restrictive cardiomyopathy
- Dysfunction in LV relaxation resulting in abnormal filling and elevated filling pressures

Current Classifications
Dilated
- Definition
- Dilation and impaired contraction of one or both ventricles resulting in an increase in total cardiac mass
- Numbers
- Incidence – 5-8 cases per 100,000 population
- Prevalence – 36 per 100,000
- STRONG HEART Study (20021) – Up to 14% of middle-aged and elderly may have asymptomatic LV dysfunction
- Causes
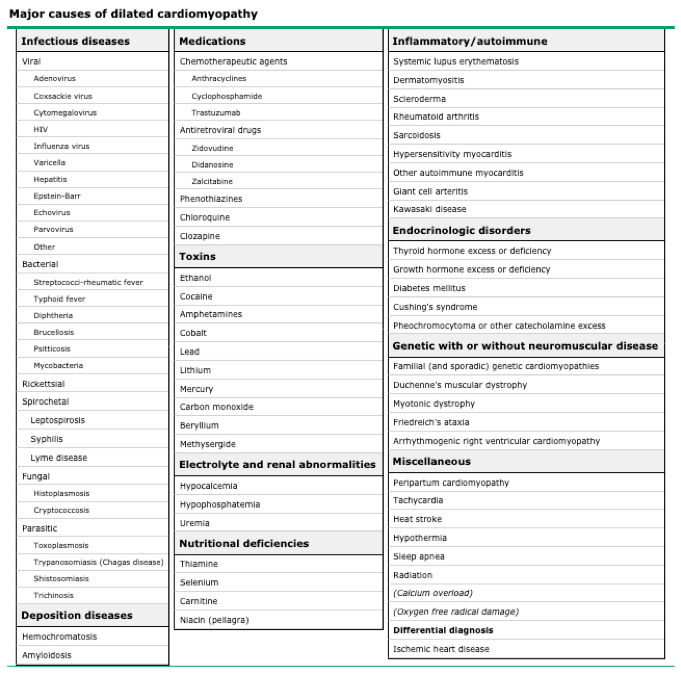
- Signs and Symptoms
- Progressive dyspnea on exertion
- Impaired exercise capacity
- Orthopnea
- Paroxysmal nocturnal dyspnea
- Peripheral edema
- Cardiomegaly
- Radiographic
- > 50% cardiothoracic ratio
- Clinical
- Displaced PMI
- S3 with gallop
- Radiographic
- Classic Echocardiographic Findings
- Left ventricular cavitary spherical dilation
- Normal to decreased wall thickness
- Reduced inward systolic motion
- Left > Right atrial enlargement and dysfunction
Hypertrophic
- Definition
- Increased Left > Right ventricular wall thickness in the absence of pathologic causing conditions
- Numbers
- Prevalence – 1:500 of the adult population
- Causes
- Primarily genetic
- Autosomal dominant with incomplete penetrance
- 60-70% of patients have mutations in the beta myosin heavy chain and cardiac myosin-binding protein C genes
- Primarily genetic
- Signs and Symptoms
- Atypical angina (25-30%)
- Presyncope and syncope during or immediately after exertion (15-20%)
- More common in patients < 30yo
- Palpitations
- Dyspnea on exertion
- Fatigue
- Clinical
- LVOT obstruction
- S4
- Harsh crescendo-decrescendo systolic murmur after S1 best heard at apex and lower left sternal border
- Accentuated by squatting and standing quickly
- Diminished by standing and squatting quickly or with handgrip
- Mitral regurgitation murmur
- LVOT obstruction
- Classic Echocardiographic Findings
- LV wall thickness > 15mm
- LV outflow obstruction > 30mmHg
- Asymmetric septal hypertrophy
- Systolic anterior motion of the mitral valve (SAM)
Restrictive
- Definition
- Non-dilated, nonhypertrophied ventricles with moderate to marked biatrial enlargement
- Numbers
- ~5% of all cases of cardiomyopathies
- Causes
- Infiltrative
- Amyloidosis, sarcoidosis
- Non-infiltrative
- Diabetic, scleroderma
- Storage Disease
- Hemochromatosis, Fabry, Gaucher
- Endomyocardial
- Cancer/Cancer therapy, pharmacologic
- Infiltrative
- Signs and Symptoms
- Dyspnea
- Peripheral edema
- Palpitations
- Fatigue
- Weakness
- Exercise intolerance
- Clinical
- Elevated JVP with a prominent y descent
- S3
- Hepatosplenomegaly and ascites
- Classic Echocardiographic Findings
- Difficult and often requires doppler interrogation
- Elevated peak mitral inflow velocity
- Rapid early mitral inflow deceleration
- Reduced annular velocity
- Normal to low diastolic volume
- Normal to low reduced LVEF
- Atrial enlargement
- Difficult and often requires doppler interrogation
The Cottage Physician (1893)


References
- Report of the WHO/ISFC task force on the definition and classification of cardiomyopathies. British heart journal. 1980; 44(6):672-3. [pubmed]
- Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation. 1996; 93(5):841-2. [pubmed]
- Maron BJ, Towbin JA, Thiene G, et al. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006; 113(14):1807-16. [pubmed]
- Elliott P, Andersson B, Arbustini E, et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. European heart journal. 2008; 29(2):270-6. [pubmed]
- Dec GW, Fuster V. Idiopathic dilated cardiomyopathy. The New England journal of medicine. 1994; 331(23):1564-75. [pubmed]
- Devereux RB, Roman MJ, Paranicas M, et al. A population-based assessment of left ventricular systolic dysfunction in middle-aged and older adults: the Strong Heart Study. American heart journal. 2001; 141(3):439-46. [pubmed]
- Felker GM, Thompson RE, Hare JM, et al. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. The New England journal of medicine. 2000; 342(15):1077-84. [pubmed]
- Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (Young) Adults. Circulation. 1995; 92(4):785-9. [pubmed]
- Maron BJ. Clinical Course and Management of Hypertrophic Cardiomyopathy. The New England journal of medicine. 2018; 379(7):655-668. [pubmed]
- Richard P, Charron P, Carrier L, et al. Hypertrophic cardiomyopathy: distribution of disease genes, spectrum of mutations, and implications for a molecular diagnosis strategy. Circulation. 2003; 107(17):2227-32. [pubmed]
- Nienaber CA, Hiller S, Spielmann RP, Geiger M, Kuck KH. Syncope in hypertrophic cardiomyopathy: multivariate analysis of prognostic determinants. Journal of the American College of Cardiology. 1990; 15(5):948-55. [pubmed]
- Muchtar E, Blauwet LA, Gertz MA. Restrictive Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy. Circulation research. 2017; 121(7):819-837. [pubmed]
- Ammash NM, Seward JB, Bailey KR, Edwards WD, Tajik AJ. Clinical profile and outcome of idiopathic restrictive cardiomyopathy. Circulation. 2000; 101(21):2490-6. [pubmed]
- Kushwaha SS, Fallon JT, Fuster V. Restrictive cardiomyopathy. The New England journal of medicine. 1997; 336(4):267-76. [pubmed]
