*** LISTEN TO THE PODCAST HERE ***






***LISTEN TO THE PODCAST HERE***

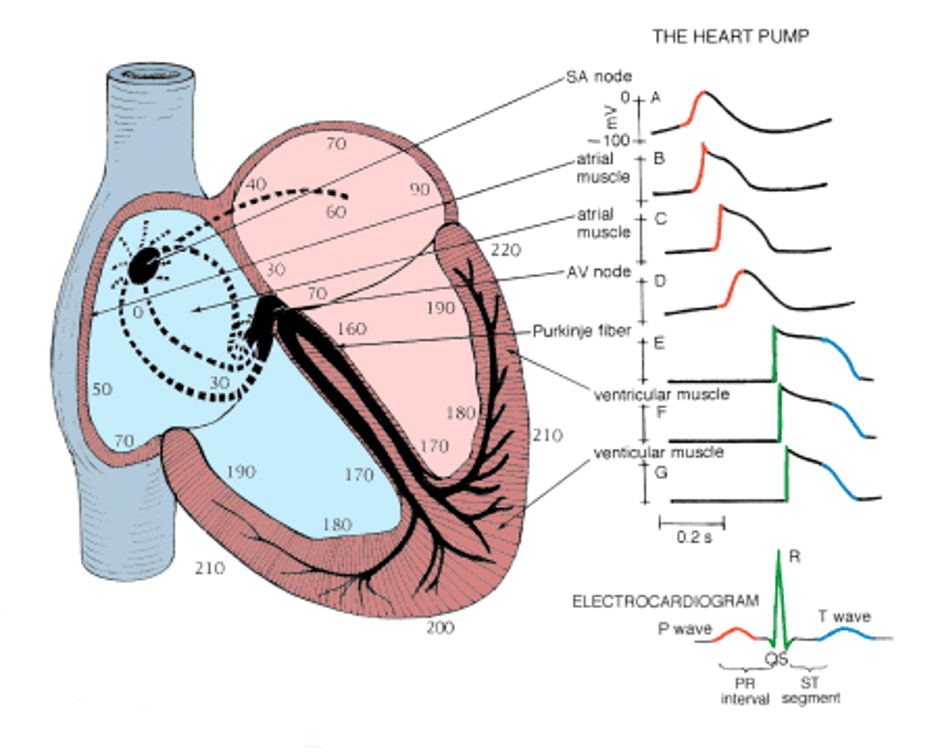
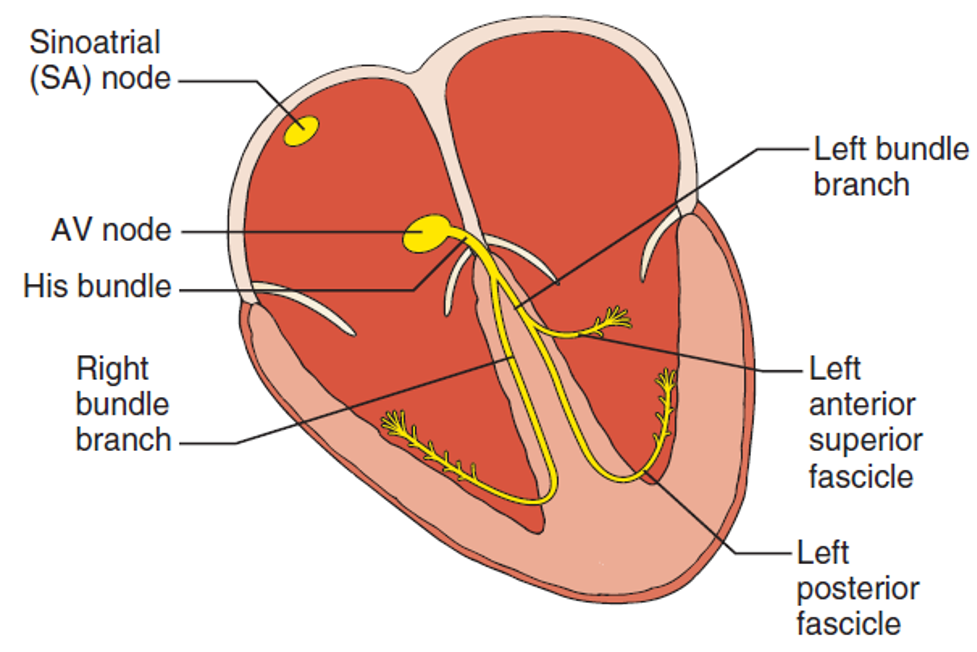
Purkinje Fibers
Other Known Aliases – subendocardial branches
Definition – specialized conducting fibers composed of electrically excitable cells located just beneath the subendocardium in the inner ventricular walls of the heart

Clinical Significance – these cells actually conduct cardiac action potentials faster and more effeciently than any other cells in the heart and are responsible for the synchronized contractions of the ventricles during depolarization. They also have intrinsic pacemaking ability at 20-40 bpm to act as a back-up pacing system.

History – Named after Jan Evangelista Purkinje (1787-1869), a Czech anatomist and experimental physiologist who received his medical doctorate from Charles University in Prague in 1818. He would be appointed Professor of Physiology in Breslau in 1823 and did revolutionary work on vision. He would later create the world’s first Department of Physiology at the University of Breslau in Prussia in 1839 and the world’s second official physiology lab in 1842. During his career of physiologic discovery and research, he discovered large neurons with branching dendrites in the cerebellum (Purkinje cells), describe the change in brightness of red and blue colors as light intensity decreases (Purkinje shift), and the eye’s reduced sensitivity to dim red light compared to dim blue light (Purkinje effect). He also was the first scientist to present work on the cellular theory of biology, the first to use the term “protoplasm” to describe the fluid in cells, and the first to report on the individuality of fingerprints. But it was in 1839 when he described his eponymous fibers of the heart. He was one of the best known scientists of his era and was so famous, people would address letters to him and simply put “Purkinje, Europe”.
References

Question
74yo woman, with a history of CAD and hyperlipidemia, presents to your office with a 6-month history of leg pain and swelling. She states that it seems to be worse when she is on her feet and improves when she can put her legs up. She denies worsening pain with activity or walking, but has recently developed a “rash” on her legs that is worrying her (see below). Physical examination reveals warmth to the feet and legs with scattered, thin hair. You appreciate 1+ DP and PT pulses bilaterally.

Bundle of His
Other Known Aliases – atrioventricular bundle
Definition – collection of electrical conduction cells of the heart that transmit impulses from the AV node to the ventricles
Clinical Significance – this bundle of cells is responsible for communication contraction impulses from the atria to the ventricles. Any damage to this area can result in varying degrees of heart block and conduction abnormalities
History – Named after Wilhelm His Jr. (1863-1934), a Swiss-born cardiologist and anatomist who received his medical doctorate from the University of Leipzig in 1889. The son of the equally famous Basel anatomist Wilhelm His Sr., he would become professor extraordinaire at his alma mater 6 year after graduating. He also went on to be physician-in-chief at the Friedrichstadt Hospital in Dresden, chair of internal medicine in Berlin, and advisory internist for several armies during World War I. He would describe his eponymous bundle as an assistant professor in 1893.
References
***LISTEN TO THE PODCAST HERE***




Question
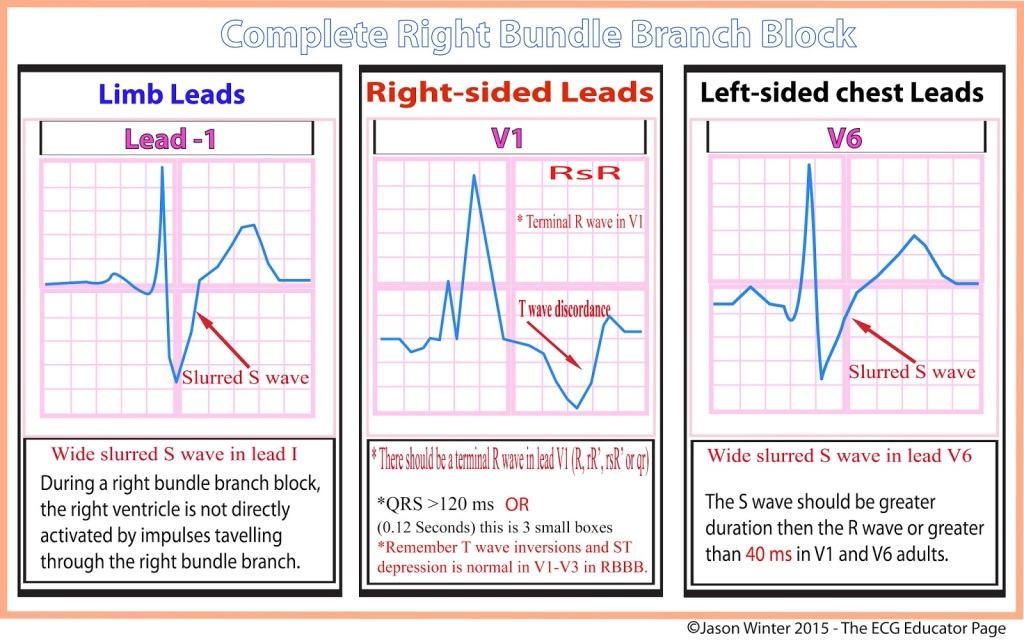
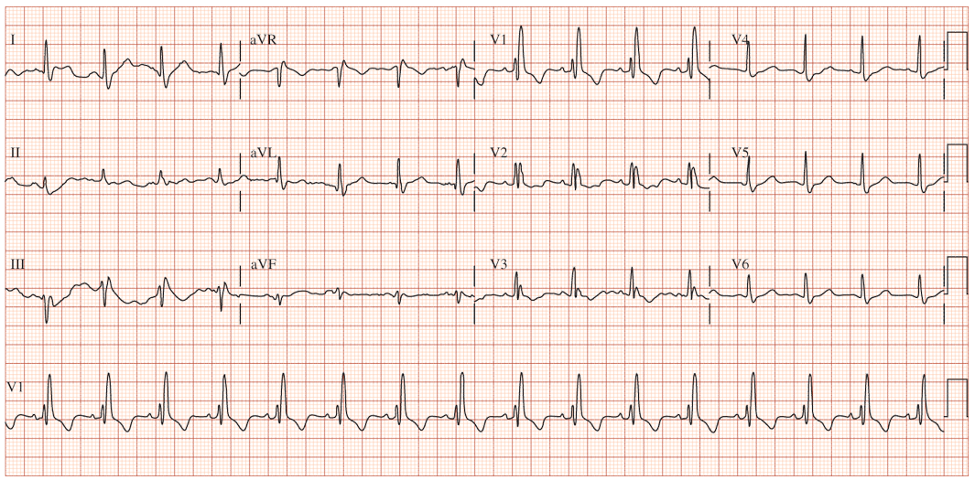
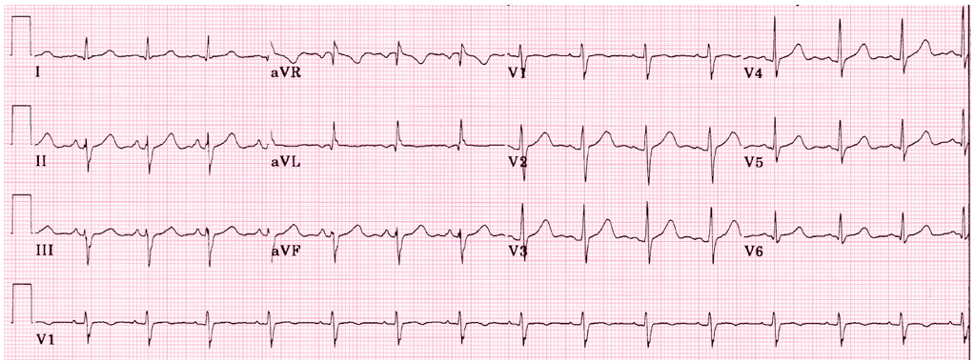
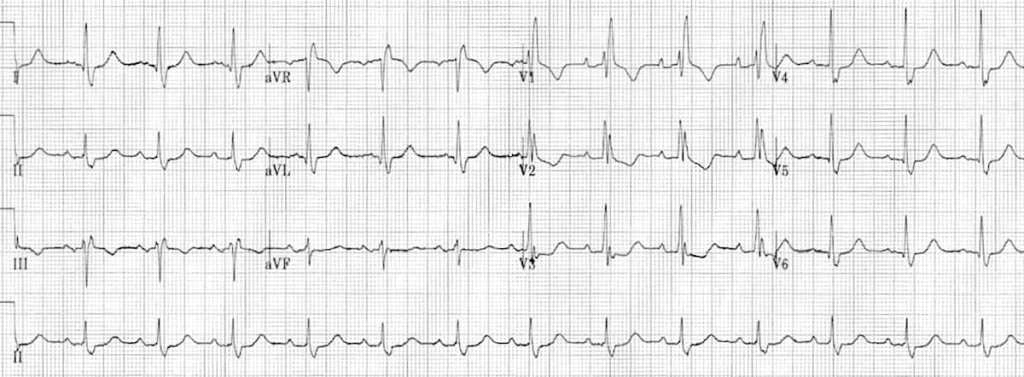
62yo man, with a history of COPD and 52-pack-year history of smoking, presents to your office to establish care. His shortness of breath has been manageable using tiotropium daily with albuterol 2-3x per month for exacerbation. He denies angina, chest pain, or unreasonable dyspnea with exertion. An EKG was performed and is below.
Answer