
Question
You get a page from a gastroenterologist asking for a consult for platelet transfusion prior to an elective colonoscopy scheduled for tomorrow. The patient is a 56yo male, with a history of ITP and HTN. This procedure is for screening purposes only and the patient has not had any melena, hematochezia, or rectal bleeding. Platelet count is 97 x 109 per liter and the rest of the CBC is within normal limits.
- Does this patient meet the platelet transfusion threshold?
- If so, how much would you transfuse?
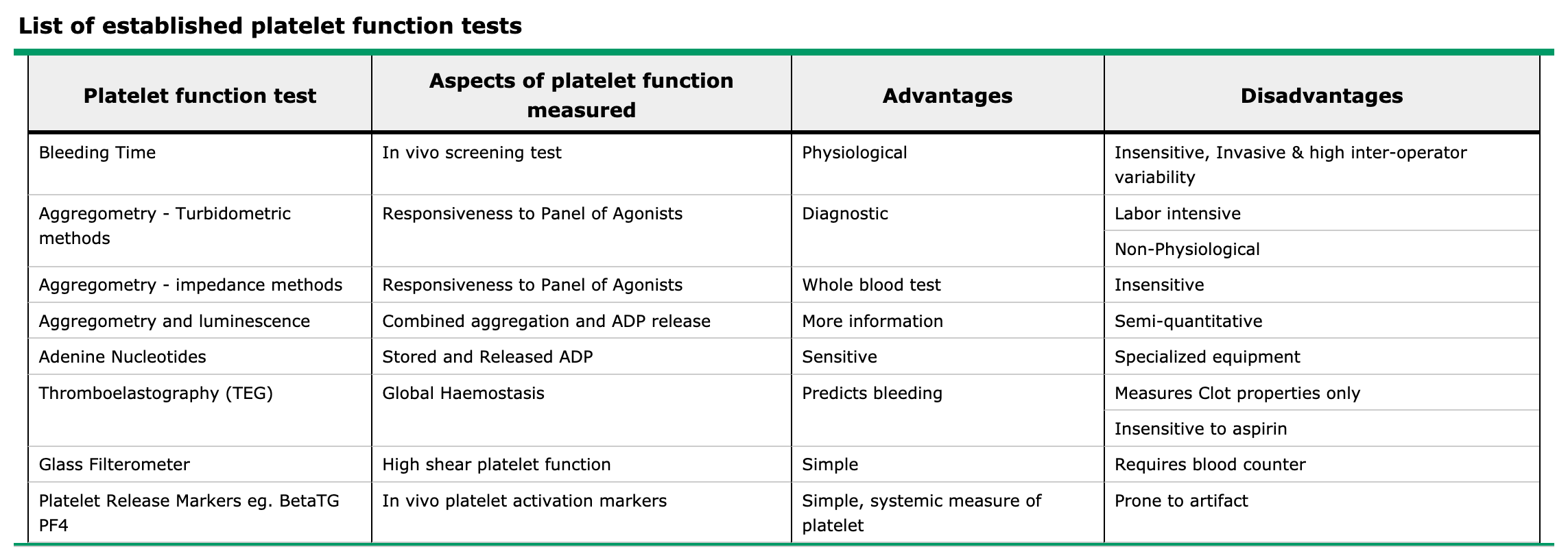
- If you were worried about bleeding, what are the other tests you could order to assess platelet function?
Answer
- The short answer is no, as he is not actively bleeding nor has any signs of anemia from chronic blood loss. Guidelines for platelet transfusions in preparation of invasive procedures is as follows:
- < 100,000/microL for neurosurgery or ocular surgery
- < 50,000/microL for most major surgery
- < 50,000/microL for therapeutic endoscopic procedures
- < 20,000/microL for low risk diagnostic endoscopic procedures
- < 30,000/microL for bronchoscopy
- < 20,000/microL for central line placement
- < 20,000/microL for lumbar puncture with hematologic malignancy
- < 50,000/microL for lumbar puncture without hematologic malignancy
- < 80,000/microL for epidural anesthesia
- < 20,000/microL for bone marrow biopsy
- The best way to assess platelet function is from a platelet function assay. This is generally determined by your facility’s lab, so it would be a good idea to talk with your lab to see what they use and how to interpret.

References
- Kumar A, Mhaskar R, Grossman BJ, et al. Platelet transfusion: a systematic review of the clinical evidence. Transfusion. 2015; 55(5):1116-27; quiz 1115. [pubmed]
- Warner MA, Woodrum D, Hanson A, Schroeder DR, Wilson G, Kor DJ. Preprocedural platelet transfusion for patients with thrombocytopenia undergoing interventional radiology procedures is not associated with reduced bleeding complications. Transfusion. 2017; 57(4):890-898. [pubmed]
