*** LISTEN TO THE PODCAST HERE ***




Pemberton Sign
Other Known Aliases – none
Definition – Raising of the patient’s arms over their head (until the arms touch their face) causes flushing and congestion of head and neck due to venous congestion and thoracic inlet obstruction.

Clinical Significance – this is a simple physical examination maneuver to diagnose a patient with superior vena cava syndrome and pressure on the thoracic inlet. A positive sign is flushing and cyanosis of the head and neck with possible respiratory distress with prolonged holding and is associated with mediastinal masses, goiters, and mediastinal lymphadenopathy.
History – Named after Hugh Spear Pemberton (1890-1956), who was an English physician and recieved his medical doctorate from the University of Liverpool in 1913. He would subsequently serve as a physician in the Royal Medical Corp during World War I and returned to Liverpool at the David Lewis Northern Hospital where he would spend his entire career. He founded one of the first diabetic clinics there in 1922 and made a name for himself in he area of endocrinology and receiving Fellowship in the Royal College of Physicians in 1941. It was in 1946 that he published a very short letter to the Lancet describing his eponymous maneuver.

References
Heinz Bodies
Other Known Aliases – Heinz-Ehrlich bodies, Ehrlich Inner Body
Definition – Deep purple small irregular bodies in red cells stained with crystal violet which represents denatured hemoglobin due to oxidative damage.
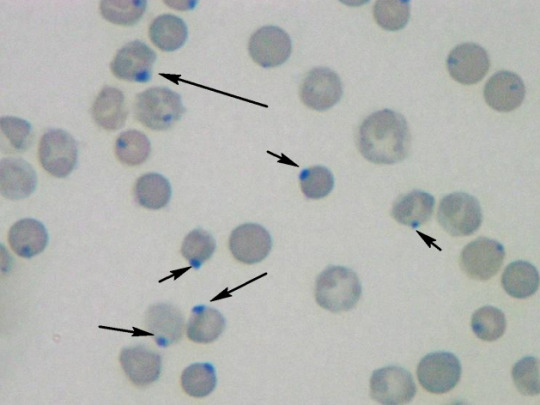
Clinical Significance – Seen in conditions with high oxidative stress such as G6PD deficiency, alpha thalassemia, NADPH deficiency, chronic liver disease, and asplenia.
History – Named after Robert Heinz (1865-1924), a German physician and pharmcologist who recieved his medical doctorate from the University of Breslau in 1888. He would work in the university chemical laboratory in Jena and Munich throughout his career studying pathology, inflammation, degeneration, and regeneration of blood. It was during this time, specifically in 1890, that he published a study on the blood of guinea pigs treated with acetylphenylhydrazine to intoduce oxidative inflammation and identified his eponymous cellular structure. Of note, Paul Ehrlich (1854-1915) is also regionally credited with identifying this structure but did not formally publish his findings.
References
von Willebrand Disease
Other Known Aliases – hereditary pseudohemophilia
Definition – Autosomal dominant, hereditary clotting disorder arising from a deficiency in the quantity and/or quality of von Willebrand factor (vWF), which is a protein required for platelet adhesion and involved in primary hemostasis. The genetic defect responsible for vWF production the vWF gene located on the short arm of chromosome 12 (12p13.2)

Clinical Significance – This is the most common type of hereditary blood-clotting disorder in humans, with 3 main hereditary types and multiple subtypes. Type 1 is the most common and often asymptomatic, Type 2 can have mild to moderate symptoms, Type 3 is the most severe and can manifest with hemarthosis and internal bleeding.
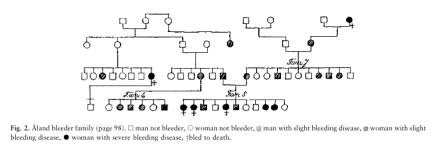
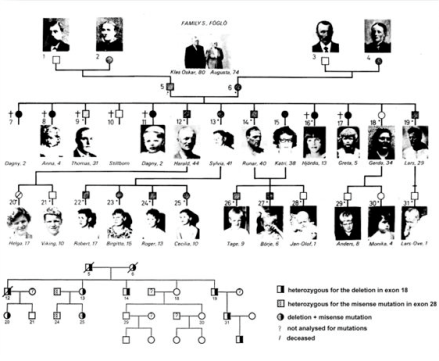
History – Named after Erik Adolf von Willebrand (1870-1949), a Finnish physician who received his medical doctorate from the University of Helsinki 1896, and who took a special interest in hematology and coagulation. In 1924, a 5yo girl was brought to him due to a bleeding disorder and he successfully performed a family history map on the girl’s 66 living family members and discovered the autosomal dominant pattern. He published his findings in 1926 in Swedish calling it “pseudo-hemophilia”, but it wasn’t until 1931 (when it was translated into German) did it gain any traction in the medical community.

References
Blumer’s Shelf
Other Known Aliases – rectal shelf
Definition – shelf-like tumor of the anterior rectal wall (Pouch of Douglas) felt on rectal examination

Clinical Significance – palpation of this “shelf” indicates implantation metastases from primary abdominal malignancy
History – Names after George Blumer (1872-1962), who was an English-American physician and recieved his medical doctorate from the Cooper Medical College (forerunner of Stanford’s medical school) in 1891. He would go onto to train under William Halstead and William Osler at Johns Hopkins Hospital at house officer. In 1906, he became professor of medicine at Yale culminating in Dean of the medical school from 1910-1920. It was during this tenure (1909) when he described his eponymous finding in an article entitled “Rectal shelf: neglected rectal sign of value in diagnosis of obscure malignant and inflammatory disease within the abdomen”.



References