Most common type of acute leukemia and the second most common type in adults
32% of all adult leukemia cases
Only 1% of all adult cancers deaths in the US
Around 12,000 deaths per year in US
3-5 cases per 100,000 population
Around 20,000 patients per year in the US get diagnosed
2% annual increase in cases from 2007-2016
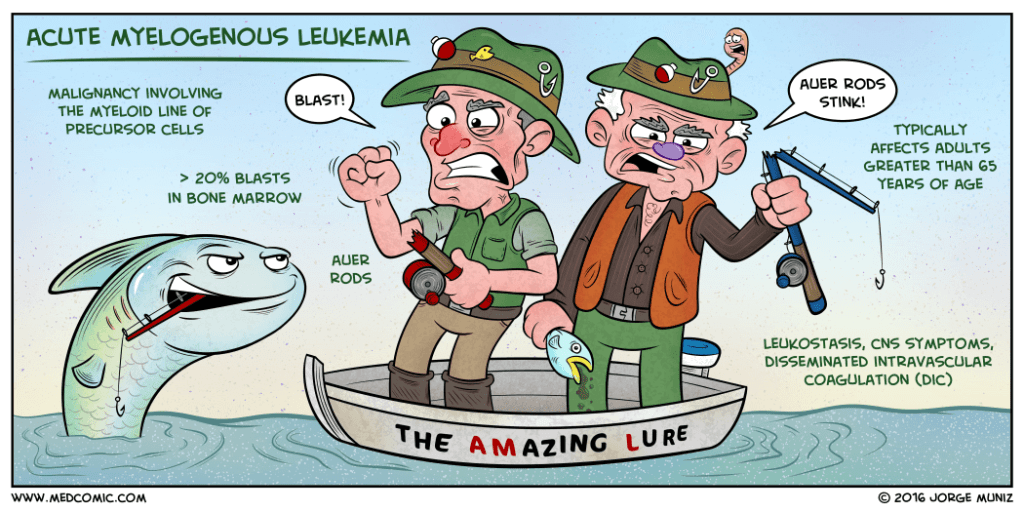
Mean age of diagnosis is 65 years and increases with age
Pathophysiology
Malignancy of myeloid precursor cells
Multipotential hematopoietic stem cell –> common myeloid progenitor –> myeloblast
2 main models
Occurs at one of several developmental stages
Occurs within the primitive multipotent cells
Two-hit hypothesis of leukemogenesis
Class I mutation
Confers a proliferative advantage
Class II mutation
Impairs hematopoietic differentiation
Mechanisms of Genetic Damage
Chemotherapy
3-5 years after alkylating agent-induced damage
Ionizing radiation
Induces double strand breaks
Typically > 20 Gy (grays)
Chemical exposure
Benzene is classically associated with AML
Infections
Human T-lymphocyte virus type I (HTLV-1
Signs and Symptoms
Constitutional
Fatigue, weakness, dyspnea
Fever
Skin (13% of patients)
Easy bruisability, ecchymoses
Pallor
HEENT
Gingival bleeding, oral candidiasis
Papilledema, retinal infiltrates
Lymphadenopathy
Abdomen (10% of patients)
Organomegaly
Spleen and liver
Musculoskeletal (4% of patients)
Polyarthritis and arthralgias
Bone pain
Emergency Presentations
Pancytopenia
Tumor lysis syndrome
Hyperkalemia, hyperphosphatemia, hyperuricemia, AKI
Bleeding
New onset CNS symptoms
Diagnostic Studies
CBC
Leukocytosis or leukopenia
20% of patients have > 100,000 cells/microL
25-40% of patients have < 5,000 cells/microL
Thrombocytopenia
75% of patients have < 100,000 cells/microL
25% of patient have < 25,000 cells/microL
Peripheral Blood
95% of patients will have circulating myeloblasts
Immature cells with large, prominent nuclei and variable amount of pale blue cytoplasms
May have Auer rods present
Myeloperoxidase reaction
Simple means of determining if the blasts are myeloid
Flow Cytometry
Can assist in detecting circulating myeloblasts
Bone Marrow Biopsy
This is the key component in the diagnosis of AML
It gives a general overview of the degree of involvement, allows for cell differential count to determine the percentage of blasts in the marrow, and provides a detailed cytologic evaluation of the blasts
Cell Origin
Identifies if myeloid, monocytic, erythroid, or megakaryocytic
Differentiates the blasts of lymphoid lineage
Infiltration
Diagnosis of AML is > 20% blasts of the total cellularity
HLA Typing in patients who are potential candidates for bone marrow transplantation
Diagnosis
Requires both of the following criteria:
Documentation of bone marrow infiltration
> 20% blasts in bone morrow
Myeloid origin
Presence of Auer rods, (+) myeloperoxidase reaction, or presence of myeloid markers on immunophenotyping
Treatment
Goals
Complete remission (<5% blasts)
Appropriate goal for most AML patients
Pretreatment evaluation
Comorbid conditions
Heart disease, renal insufficiency, liver disease
Physical function and performance status
ECOG Scale most commonly used
Two distinct treatment phases
Induction
Combination therapy (7 and 3 regimen)
Cytarabine
Interferes with DNA synthesis
7 day continuous infusion
Anthracycline
Daunorubicin, idarubicin
Inhibition of topoisomerase II
Leads to DNA breaks
Day 1, 2, and 3
Bone marrow biopsy 7-10 days after induction to re-assess
Postremission management
Continuing chemotherapy
Hematopoietic cell transplant
Prognosis
Overall 5-year survival is 15%
Decreases with age
53% 5-year survival in 15-24yo to 13% in 70-79yo
Genetic subtypes
Karyotypes
Gene mutations
The Cottage Physician (1893)
References
Acute myeloid leukemia statistics. Cancer.net. Accessed on 03/22/2020 [link]
Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA: a cancer journal for clinicians. 2017; 67(1):7-30. [pubmed]
Reilly JT. Pathogenesis of acute myeloid leukaemia and inv(16)(p13;q22): a paradigm for understanding leukaemogenesis? British journal of haematology. 2005; 128(1):18-34. [pubmed]
Levine EG, Bloomfield CD. Leukemias and myelodysplastic syndromes secondary to drug, radiation, and environmental exposure. Seminars in oncology. 1992; 19(1):47-84. [pubmed]
Shuryak I, Sachs RK, Hlatky L, Little MP, Hahnfeldt P, Brenner DJ. Radiation-induced leukemia at doses relevant to radiation therapy: modeling mechanisms and estimating risks. Journal of the National Cancer Institute. 2006; 98(24):1794-806. [pubmed]
Austin H, Delzell E, Cole P. Benzene and leukemia. A review of the literature and a risk assessment. American journal of epidemiology. 1988; 127(3):419-39. [pubmed]
Shah A, Andersson TM, Rachet B, Björkholm M, Lambert PC. Survival and cure of acute myeloid leukaemia in England, 1971-2006: a population-based study. British journal of haematology. 2013; 162(4):509-16. [pubmed]








Pingback: PAINE PANCE Postcard – Acute Lymphoblastic Leukemia | PAINE Podcast and Medical Blog