

***LISTEN TO THE PODCAST HERE***
Classifications and Subtypes
- 3rd Edition of the International Classification of Headache Disorders (ICHD-3)
- Primary Headaches
- Secondary Headaches
- Neuropathies, Facial Pains, and Other Headaches
- 90% of headaches fall into 3 primary headache categories
Migraines

Tension-Type

Trigeminal Autonomic Cephalgias

Approach to Evaluation
- Malignancy of myeloid precursor cells
- Multipotential hematopoietic stem cell –> common myeloid progenitor –> myeloblast
Signs and Symptoms
- Environment
- Turn off the lights
- Speak quiet
- Let the patient talk uninterrupted about what is going on
- History
- Age of onset
- Past medical and family history
- Medication history
- Presence of absence of aura
- Characteristics
- Frequency
- Intensity
- Duration
- Onset
- Quality
- Location
- Radiation
- Number of headaches per month
- Associated symptoms
- Fever, nausea, vomiting, visual disturbances, dizziness, syncope
- Precipitating, exacerbating or relieving factors
- Positional changes, exertional
- Photophobia, phonophobia
- Relationship to food or alcohol
- Women
- Contraception
- Associated with menstrual cycle
- Physical Examination
- Review of vital signs
- Auscultate for bruits (evaluation for AVM)
- Neck, eyes, head
- Palpate head, neck, and shoulder regions
- Palpate neck and head arteries
- Palpate neck muscles for spasms or tightness
- Neurologic examination
- Mental status
- Cranial nerve evaluation
- Fundoscopy
- Motor and sensory examination
- Cerebellar exam, including gait, Romberg
Concerning History and Physical Examination Findings
- SNNOOP10 Red Flag List
- Systemic symptoms
- Fever
- Neoplasm history
- Neurologic deficits
- Focal or general
- Onset
- Sudden or abrupt
- Older age
- Age > 50 years
- Pattern change or recent new headache
- Positional
- Precipitation
- Sneezing, coughing, exercise, exertional
- Papilledema
- Progressive headache and atypical presentations
- Pregnancy or postpartum
- Painful eye with autonomic features
- Post-traumatic
- Pathology of the immune system
- Painkiller overuse
- Systemic symptoms
- Presence of ANY of the SNNOOP10 require further investigation
- Low-Risk Documentation Pearls
- Age < 50 years
- Features typical of primary headache
- History of similar headache
- No abnormal neurological findings
- No concerning change in usual headache pattern
- No high-risk comorbid conditions
- No new or concerning findings on physical examination
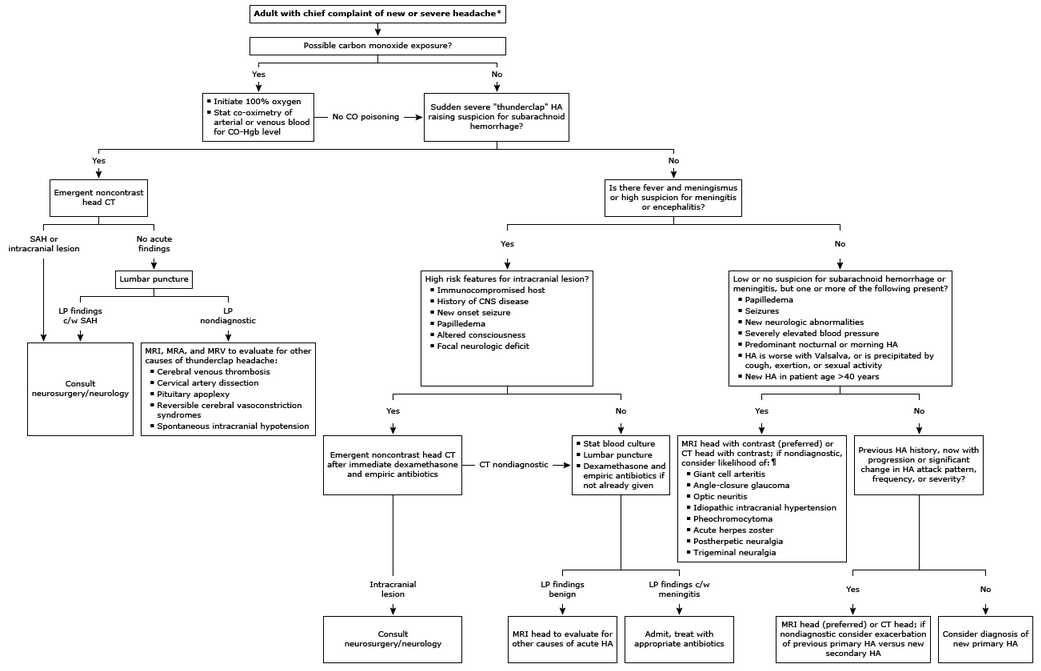
Serious and/or Life-Threatening Headaches
- “Thunderclap”
- sudden onset, maximal intensity

- Neck pain with Horner’s Syndrome and/or neurologic deficit
- Cervical artery dissection
- Fever, AMS, and/or nuchal rigidity
- Meningitis, encephalitis
- Neurologic deficit and/or papilledema
- Increased intracranial pressure
- Pseudotumor cerebri, mass effect lesion
- Increased intracranial pressure
- Orbital or periorbital symptoms
- Acute angle closure glaucoma, cavernous sinus thrombosis/fistula
Imaging Recommendations
- Criteria for imaging in Headaches
- Any of the SNNOOP10 findings
- Emergency Setting
- CT is generally the study of choice because:
- Widely available
- Most life-threatening conditions are seen on CT
- Safer for unstable patients
- MRI is an option if:
- New headache with optic disc edema
- Chronic headache with new features
- Known or suspected cancer
- Patient is pregnant
- CT is generally the study of choice because:
- Outpatient Setting
- American Academy of Neurology recommend imaging for:
- Patients with unexplained abnormal finding on neurologic examination
- Patients with atypical headache features or headaches that don’t fulfill strict definition of other primary headache disorder
- Choosing Wisely Campaign – MRI is recommended over CT
- Consult radiology for recommendations of type of study
- Imaging vessels, facial structures, orbits
- American Academy of Neurology recommend imaging for:
Indications for Lumbar Puncture
- Suspicion of SAH with a negative CT
- Suspicion of infectious or inflammatory pathology
- Suspicion of pseudotumor cerebri
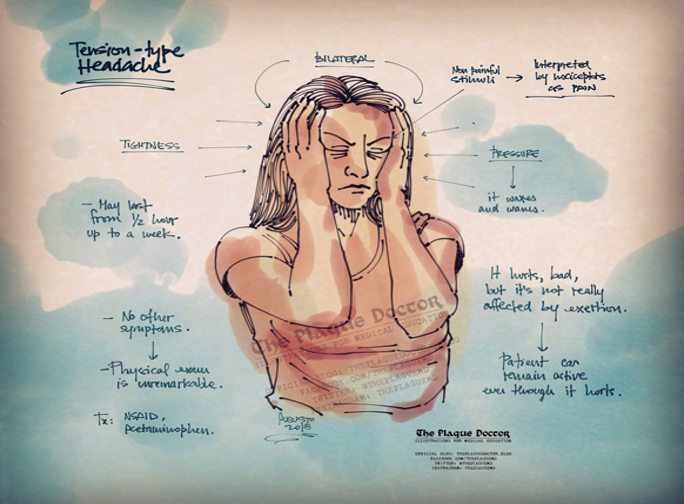
Tension-Type Headache
Epidemiology
- Most common headache subtype
- 2nd most prevalent disorder in the world
- Slightly more prevalent in women
- Least distinct of the primary subtypes
- Least studied
Classifications
- Episodic
- Infrequent – < 1 episode per month
- Frequent – 1-14 episodes per month
- Chronic – 15 or more episodes per month
Pathophysiology
- Peripheral activation or sensitization of the myofascial nociceptors leading to heightened sensitivity of the pain pathways in the central nervous system
- Central factors
- Increased pain sensitivity
- Altered brainstem and limbic-controlled descending pain systems
- Peripheral factors
- Muscular abnormalities
- Trigger points, postural, mobility
- Muscular abnormalities
- Central factors
Clinical Features
- History
- Quality
- Dull, pressure, fullness, band-like, weight on shoulders
- Increased stress and mental tension
- Pericranial muscular tenderness
- Masseter, temporalis, sternocleidomastoid, trapezius
- Quality
Diagnostic Criteria
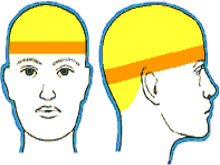
- Two of the following:
- Bilateral location
- Pressing/tightening, non-pulsatile quality
- Mild/moderate intensity
- Not aggravated by routine physical activity
- Both of the following
- No more than one of photophobia or phonophobia
- No moderate/severe nausea or vomiting
- Episodic
- At least 10 episodes lasting 30 minutes to 7 days
- Chronic
- At least 15 episodes per month for at least 3 months lasting for hours to days
Treatment
- Acute/Abortive
- NSAID Analgesia
- Ibuprofen, acetaminophen, aspirin
- Can be combined with caffeine
- Triptans can be used if NSAIDs fail
- NSAID Analgesia
- Preventative
- Antidepressants
- Tricyclic antidepressants
- Amitriptyline has the best evidence
- Start 10mg and increased 10mg every 2-3 weeks until:
- Improvement of headaches
- Max dose of 125mg/day
- Start 10mg and increased 10mg every 2-3 weeks until:
- Amitriptyline has the best evidence
- Mirtazapine and venlafazine has some limited data
- Tricyclic antidepressants
- Anticonvulsants
- Topiramate and gabapentin can also be helpful
- Trigger point injections
- Botulinum toxin injections
- Behavioral treatments
- Cognitive-behavioral therapy
- Relaxation techniques
- Biofeedback
- Acupuncture and physical therapy has limited evidence of success
- Antidepressants

Migraines

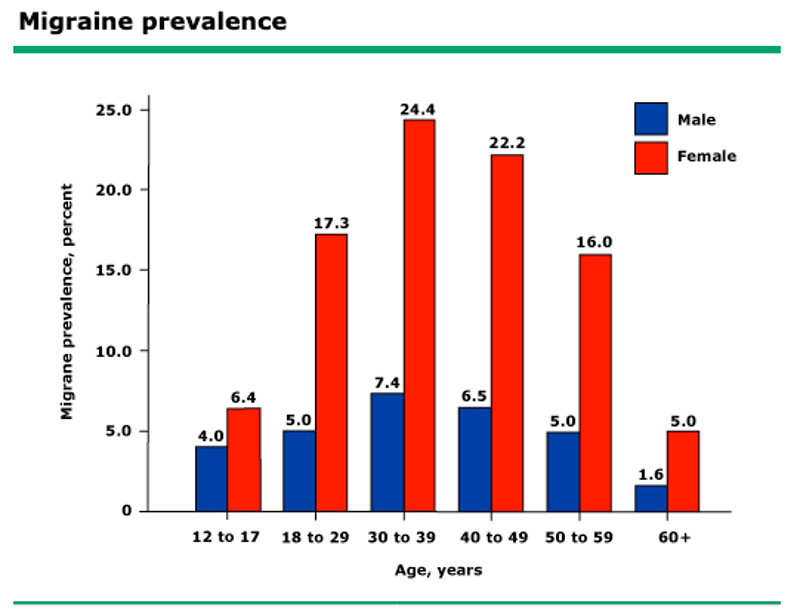
Epidemiology
- Affects up to 12% of the population
- More frequent in women
- Most common age range is 30-40 years
Pathophysiology
- Cortical spreading depression
- Self-propagating wave of neuronal and glial depolarization that spreads across the cerebral cortex
- This then causes:
- Aura
- Activation of the trigeminovascular system
- Causes inflammatory changes in the pain-sensitive meninges
- Increase pain sensitization
- Alters blood-brain barrier permeability


Clinical Features
- Cascade of four events over a course of hours to days:
- Prodrome
- 24-48 before headache
- Yawning, euphoria, depression, irritability, food cravings
- Aura
- 25% of patient experience focal neurologic symptom
- Visual
- Positive
- Lines, shapes, objects
- Negative
- Scintillating scotomas, vision loss
- Positive
- Sensory
- Positive
- Burning, paresthesias
- Negative
- numbness
- Positive
- Auditory
- Positive
- Tinnitus, noises
- Negative
- Hearing loss
- Positive
- Visual
- 25% of patient experience focal neurologic symptom
- Headache
- Unilateral
- Throbbing, pulsatile quality
- Nausea or vomiting common
- Photophobia and phonophobia common
- Prodrome
- Feeling of exhaustion, elation, euphoria
- Prodrome


Precipitating Factors or Triggers

Diagnostic Criteria
- Without an Aura
- ≥ 5 attacks with the following:
- Lasting 4-72 hours
- Headache as 2 of the following:
- Unilateral
- Pulsating quality
- Moderate/severe
- Aggravation by exertion
- ≥ 1 of the following:
- Nausea or vomiting
- Photophobia or phonophobia
- ≥ 5 attacks with the following:
- With an Aura
- ≥ 2 attacks with the following:
- ≥ 1 of the following reversible aura symptoms:
- Visual
- Sensory
- Speech
- Motor
- Brainstem
- Retinal
- ≥ 1 of the following reversible aura symptoms:
- ≥ 2 of the following:
- Aura spreads and/or 2 or more occur in succession
- Each aura lasts 5-60 min
- At least 1 aura is unilateral
- Aura is accompanied or followed by headache within 60 min
- ≥ 2 attacks with the following:
Treatment
- Acute/Abortive Therapy
- Without nausea or vomiting
- NSAIDs
- With nausea or vomiting
- Triptans
- Sumatriptan
- SQ 6mg
- IN 20mg
- Sumatriptan
- Antiemetics
- Metoclopramide 10mg
- Prochlorperazine 10mg
- Dihydroergotamine 1mg IM/SQ
- Generally combined with metoclopromide
- Dexamethasone 10mg IM
- More for prevention of migraine recurrence
- Triptans
- Without nausea or vomiting
- Preventative Therapy
- Think about compelling indications and concomitant diseases
- Antihypertensives
- Beta Blockers
- Metoprolol, propranolol
- Calcium Channel Blockers
- Verapamil, flunarizine
- ACE/ARB
- Lisinopril, candesartan
- Beta Blockers
- Antidepressants
- Amitriptyline, venlafaxine
- Anticonvulsants
- Topiramate, valproate, gabapentin
- Calcitonin Gene-Related Peptide (CGRP) Antagonist
- Erenumab, fremanezumab, galcanezumab
- Acupuncture, nerve stimulation

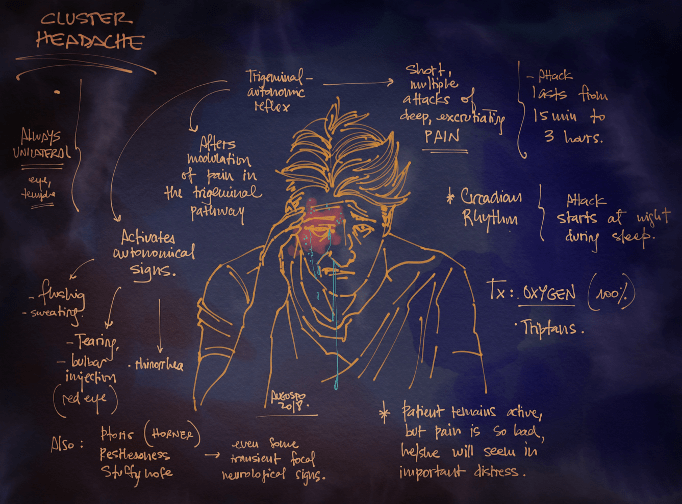
Cluster
Epidemiology
- <1% of headaches
- Men > women
Pathophysiology
- Complex and incompletely understood
- Most widely accepted theory
- Hypothalamic activation with secondary activation of the trigeminal-autonomic reflex
- Most widely accepted theory
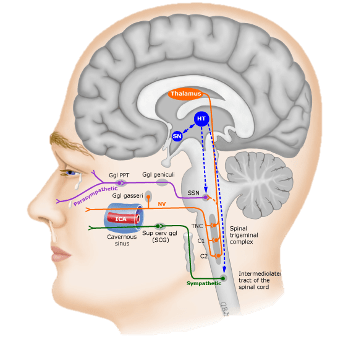
Clinical Features
- Unilateral attacks of severe orbital, supraorbital, or temporal pain
- Autonomic phenomena
- Ptosis, miosis, lacrimation, conjunctival injection, rhinorrhea, nasal congestion
- Only occur during the episode
- Ipsilateral to the pain site
- Ptosis, miosis, lacrimation, conjunctival injection, rhinorrhea, nasal congestion
- Circadian periodicity
- Occur daily for several weeks and then remit for up to a year
- Autonomic phenomena

Diagnostic Criteria
- At least five attacks characterized by severe unilateral orbital, supraorbital, or temporal pain lasting 15-180 minutes with at least one of the following:
- Conjunctival injections and/or lacrimation
- Nasal congestion and/or rhinorrhea
- Eyelid edema
- Forehead and facial sweating
- Miosis and/or ptosis
- Sense of restlessness or agitation
- Classification
- Episodic
- Occur in circardian periodicity in clusters
- At least two cluster periods lasting 7 days to one year separated by a pain-free remission of at least 3 months
- Occur in circardian periodicity in clusters
- Chronic
- Attacks occur without a remission period or remission lasting less than 3 months
- Episodic
- Imaging
- Initial event warrants an MRI to rule-out intracranial pathology that also can cause autonomic dysfunction
Treatment
- Acute/Abortive Therapy
- 100% oxygen via non-rebreather
- SQ sumatriptan 6mg
- IN lidocaine 4-10% 1mL
- Ergot-derivitives
- Octreotide 100mcg SQ
- Preventative Therapy
- Verapamil 240mg daily
- Bridge with prednisone 60-100mg daily for 5 days, with a 10mg/day taper
- Galcanezumab can be used for chronic
- Lithium has limited data
- Topiramate can be used as add-on therapy
- Verapamil 240mg daily


The Cottage Physician (1893)

References
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia : an international journal of headache. 2018; 38(1):1-211. [pubmed]
- Goadsby PJ. Migraine and Other Primary Headache Disorders. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com.ezproxy.uthsc.edu/content.aspx?bookid=2129§ionid=192532155 . Accessed May 03, 2020.
- Koyfman A, Long B. Headache. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com.ezproxy.uthsc.edu/content.aspx?bookid=2353§ionid=189593946 . Accessed May 03, 2020.
- Hainer BL, Matheson EM. Approach to acute headache in adults. American family physician. 2013; 87(10):682-7. [pubmed]
- Do TP, Remmers A, Schytz HW, et al. Red and orange flags for secondary headaches in clinical practice: SNNOOP10 list. Neurology. 2019; 92(3):134-144. [pubmed]
- Lyrer PA, Brandt T, Metso TM, et al. Clinical import of Horner syndrome in internal carotid and vertebral artery dissection. Neurology. 2014; 82(18):1653-9. [pubmed]
- Loder E, Weizenbaum E, Frishberg B, Silberstein S, . Choosing wisely in headache medicine: the American Headache Society’s list of five things physicians and patients should question. Headache. ; 53(10):1651-9. [pubmed]
- Jensen RH. Tension-Type Headache – The Normal and Most Prevalent Headache. Headache. 2018; 58(2):339-345. [pubmed]
- Martelletti P, Birbeck GL, Katsarava Z, Jensen RH, Stovner LJ, Steiner TJ. The Global Burden of Disease survey 2010, Lifting The Burden and thinking outside-the-box on headache disorders. The journal of headache and pain. 2013; 14:13. [pubmed]
- Bendtsen L. Central sensitization in tension-type headache–possible pathophysiological mechanisms. Cephalalgia : an international journal of headache. 2000; 20(5):486-508. [pubmed]
- Moore RA, Derry S, Wiffen PJ, Straube S, Bendtsen L. Evidence for efficacy of acute treatment of episodic tension-type headache: methodological critique of randomised trials for oral treatments. Pain. 2014; 155(11):2220-8. [pubmed]
- Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007; 68(5):343-9. [pubmed]
- Laurell K, Artto V, Bendtsen L, et al. Premonitory symptoms in migraine: A cross-sectional study in 2714 persons. Cephalalgia : an international journal of headache. 2016; 36(10):951-9. [pubmed]
- Kelman L. The triggers or precipitants of the acute migraine attack. Cephalalgia : an international journal of headache. 2007; 27(5):394-402. [pubmed]
- Marmura MJ, Silberstein SD, Schwedt TJ. The acute treatment of migraine in adults: the american headache society evidence assessment of migraine pharmacotherapies. Headache. 2015; 55(1):3-20. [pubmed]
- Nesbitt AD, Goadsby PJ. Cluster headache. BMJ (Clinical research ed.). 2012; 344:e2407. [pubmed]
- May A, Schwedt TJ, Magis D, Pozo-Rosich P, Evers S, Wang SJ. Cluster headache. Nature reviews. Disease primers. 2018; 4:18006. [pubmed]
- Obermann M, Holle D, Naegel S, Burmeister J, Diener HC. Pharmacotherapy options for cluster headache. Expert opinion on pharmacotherapy. 2015; 16(8):1177-84. [pubmed]
- Francis GJ, Becker WJ, Pringsheim TM. Acute and preventive pharmacologic treatment of cluster headache. Neurology. 2010; 75(5):463-73. [pubmed]
