

***LISTEN TO THE PODCAST HERE***
Pleural Anatomy and Physiology
- 2 types of pleura in the thorax
- Parietal pleura
- Which covers the chest wall and diaphragm
- 30-40 micrometers thick
- Contains lymphatic stomata
- Holes between the mesothelial and subpleural layers that allow for drainage into the lymphatic system
- Contains intercostal microvessels
- Produce interpleural fluid
- Visceral pleura
- Which covers the lung parenchyma
- 20-80 micrometers thick
- Contain bronchial microvessels
- Arise from pulmonary veins and produce interpleural fluid
- Parietal pleura
- The interpleural space is between them and produces 0.1-0.2 mL/kg (10-20 mL per hemithorax) of fluid to keep these pleura from adhering to each other and maintain lubrication
- This fluid is constantly produced (0.01 mL/kg/hr) and absorbed
- Originates from the systemic pleural microvessels
- Theorized that parietal is more important
- Intercostal microvessels are closer to the interpleural space
- Higher filtration pressure than pulmonary veins
- Theorized that parietal is more important
- Dependent on balance of hydrostatic pressure opposed by the counterbalancing osmotic pressure and membrane permeability
- Transudative fluid collection
- Increased hydrostatic pressure
- Decreased oncotic pressure
- Exudative fluid collection
- Decreased pleural membrane permeability
- Lymphatic blockage
- Transudative fluid collection


Associated Diseases and Causes

Clinical Presentation
- Symptoms
- Patients can be asymptomatic, have fluid specific symptoms, and have disease specific symptoms
- Fluid specific
- Dyspnea
- Cough
- Pleuritic chest pain
- Disease specific
- Fever, hemoptysis, orthopnea, peripheral edema, weight changes, ascites
- Physical Examination
- Fluid specific
- Decreased or asymmetric chest wall movement
- Decreased breath sounds
- Dullness to percussion
- Decreased tactile fremitus
- Pleural friction rub
- (+) egophony
- Disease specific
- Crackles, JVD, hepatosplenomegaly, lymphadenopathy, S3 gallop, pitting edema,
- Fluid specific
Imaging in Suspected Pleural Effusions
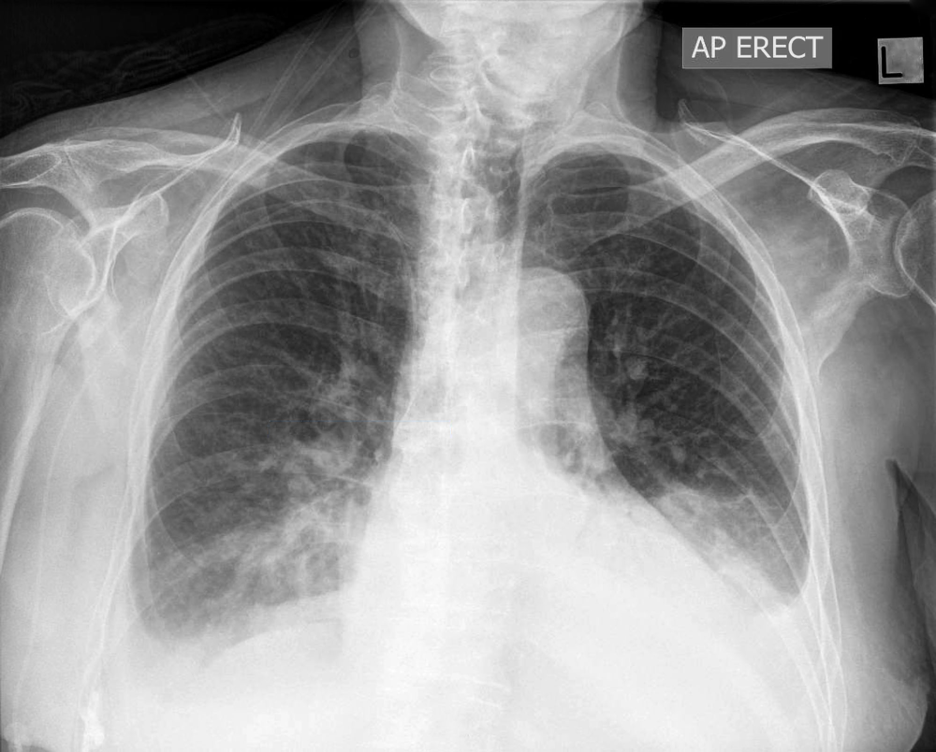
- Chest Radiograph
- Blunting of the costophrenic angle
- At least 150mL needed on PA
- At least 50mL needed on lateral decubitus
- At least 500mL needed for diaphragm obliteration
- Blunting of the costophrenic angle
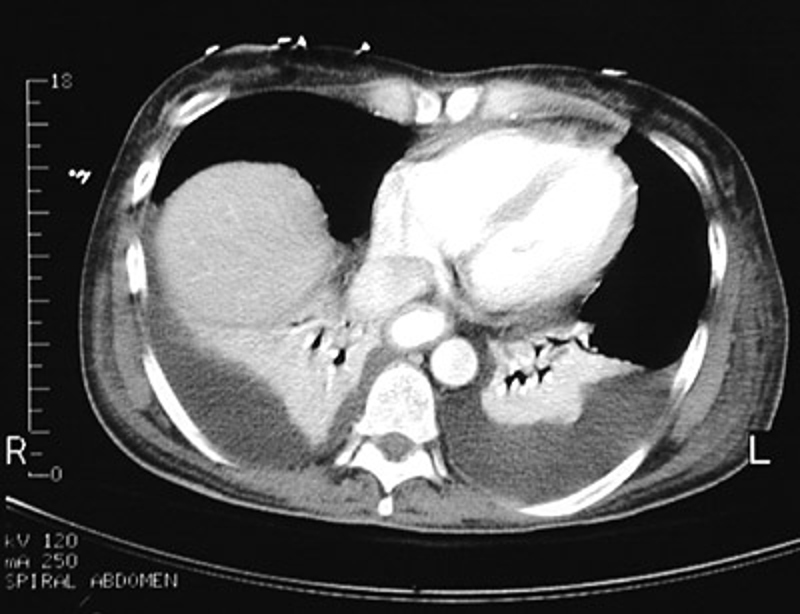
- Computed Tomography
- Can detect as little as 2mL of fluid
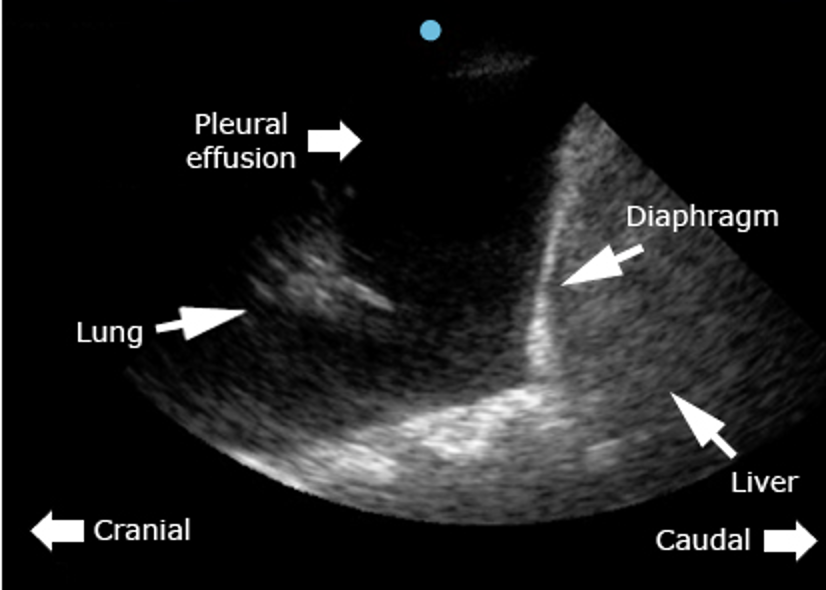
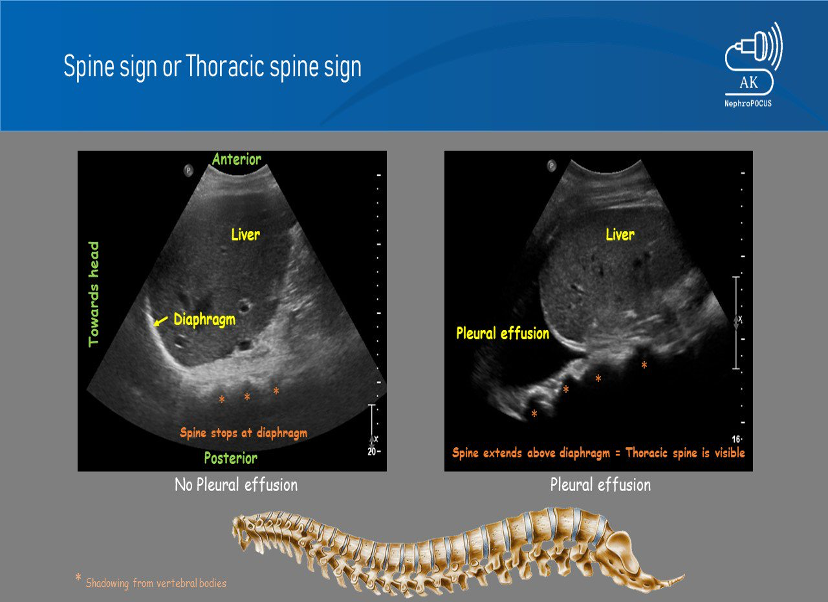
- Ultrasound
- Can detect as little as 20mL
- Phased array probe with patient sitting upright
- Scan posterior/lateral caudal to cranial to find fluid line
- (+) spine sign
Thoracentesis
- Once the diagnosis is made, a thoracentesis needs to be performed for biochemical fluid analysis
Fluid Analysis
- Routine fluid labs
- Cell count and differential
- pH
- Protein
- LDH
- Glucose
- Cholesterol
- Non-routine
- N-terminal BNP
- Triglycerides
- Creatinine
- Amylase
- Cancer-related biomarkers
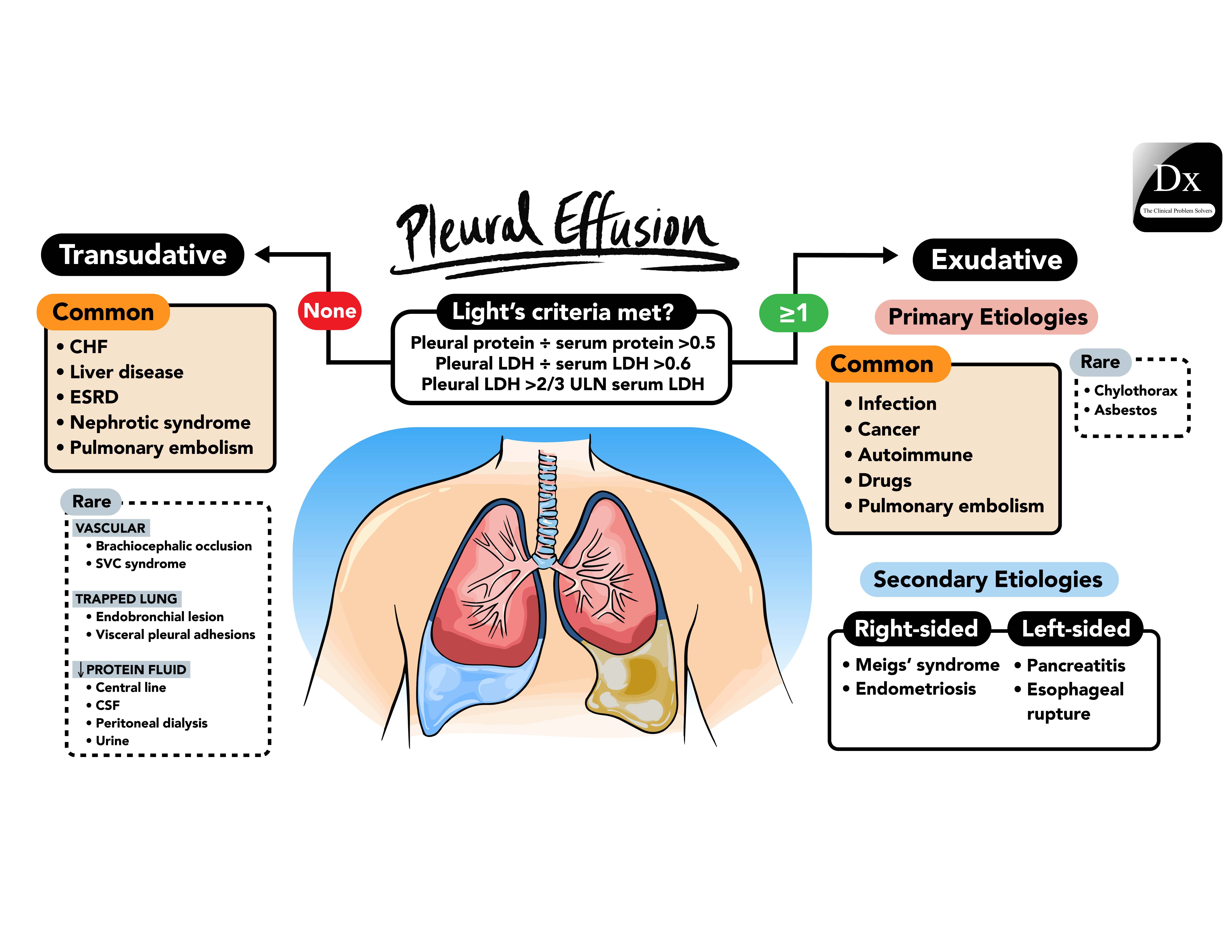
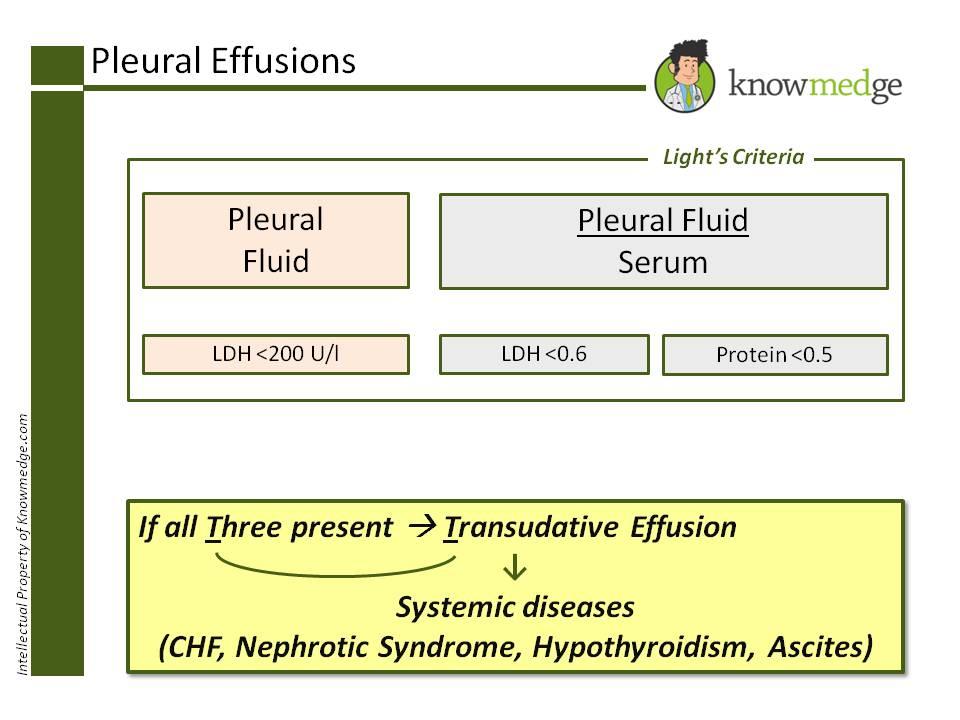
- Lights Criteria
- Exudative if one (1) of following present:
- Pleural/serum protein ratio > 0.5
- Pleural/serum LDH > 0.6
- Pleural fluid LDH > 2/3rd ULN of serum LDH
- Lights Criteria Criticism
- Needs both pleural fluid and serum
- Newer studies use only pleural fluid
- Exudative if one (1) of the following:
- Pleural fluid cholesterol > 45 mg/dL
- Pleural fluid protein > 2.6 g/dL
- Pleural fluid LDH > 0.45x ULN of serum LDH
- Exudative if one (1) of the following:
- Exudative if one (1) of following present:
Treatment
- Non-malignant effusions
- Treat underlying condition
- Repeated drainage for symptomatic patients
- If persistent:
- Repeat thoracentesis as needed
- Revisit primary diagnosis
- Consider pleurodesis
- Chemical
- Talc slurry or doxycycline through chest tube
- Mechanical
- VATS
- Chemical
- Indwelling pleural catheter
- Reserved for patients who decline, fail, or not candidates for pleurodesis
- Malignant effusions
- Can be complicated

Cottage Physician (1898)

References
- Lai-Fook SJ. Pleural mechanics and fluid exchange. Physiol Rev. 2004; 84(2):385-410. [pubmed]
- Jantz MA, Antony VB. Pathophysiology of the pleura. Respiration. 2008; 75(2):121-33. [pubmed]
- Feller-Kopman D, Light R. Pleural Disease. N Engl J Med. 2018; 378(8):740-751. [pubmed]
- http://www.meddean.luc.edu/lumen/MedEd/medicine/pulmonar/apd/plep.htm
- Saguil A, Wyrick K, Hallgren J. Diagnostic approach to pleural effusion. Am Fam Physician. 2014; 90(2):99-104. [pubmed]
- Wong CL, Holroyd-Leduc J, Straus SE. Does this patient have a pleural effusion? JAMA. 2009; 301(3):309-17. [pubmed]
- Chesnutt AN, Chesnutt MS, Prendergast NT, Prendergast TJ. Pleural Effusion. In: Papadakis MA, McPhee SJ, Rabow MW. eds. Current Medical Diagnosis and Treatment 2020. McGraw-Hill; Accessed July 05, 2020. https://accessmedicine-mhmedical-com.ezproxy.uthsc.edu/content.aspx?bookid=2683§ionid=225058693
- Light RW. Disorders of the Pleura. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e. McGraw-Hill; Accessed July 05, 2020. https://accessmedicine-mhmedical-com.ezproxy.uthsc.edu/content.aspx?bookid=2129§ionid=192031615
- Moskowitz H, Platt RT, Schachar R, Mellins H. Roentgen visualization of minute pleural effusion. An experimental study to determine the minimum amount of pleural fluid visible on a radiograph. Radiology. 1973; 109(1):33-5. [pubmed]
- Radiopaedia. Pleural Effusions. https://radiopaedia.org/articles/pleural-effusion?lang=us
- Gonlugur U, Gonlugur TE. The distinction between transudates and exudates. J Biomed Sci. 2005; 12(6):985-90. [pubmed]
- Heffner JE, Brown LK, Barbieri CA. Diagnostic value of tests that discriminate between exudative and transudative pleural effusions. Primary Study Investigators. Chest. 1997; 111(4):970-80. [pubmed]
- Steger V, Mika U, Toomes H, et al. Who gains most? A 10-year experience with 611 thoracoscopic talc pleurodeses. Ann Thorac Surg. 2007; 83(6):1940-5. [pubmed]
- Patil M, Dhillon SS, Attwood K, Saoud M, Alraiyes AH, Harris K. Management of Benign Pleural Effusions Using Indwelling Pleural Catheters: A Systematic Review and Meta-analysis. Chest. 2017; 151(3):626-635. [pubmed]
- Feller-Kopman DJ, Reddy CB, DeCamp MM, et al. Management of Malignant Pleural Effusions. An Official ATS/STS/STR Clinical Practice Guideline. Am J Respir Crit Care Med. 2018; 198(7):839-849. [pubmed]
- Bibby AC, Dorn P, Psallidas I, et al. ERS/EACTS statement on the management of malignant pleural effusions. Eur Respir J. 2018; 52(1):. [pubmed]
