

***LISTEN TO THE PODCAST HERE***
Epidemiology
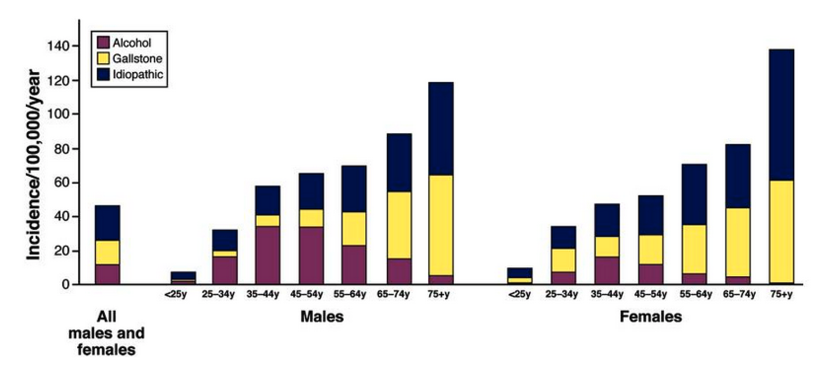
- 13-45 per 100,000 person incidence in the US
- Most common GI cause of hospital admission in the US
- > 300,000 per year
- Average 4-day stay with cost > $6000/case
- Equal gender representation across the lifespan
- Alcohol pancreatitis more common in men
- 2-3 fold higher rates in African Americans
Risk Factors and Etiologies
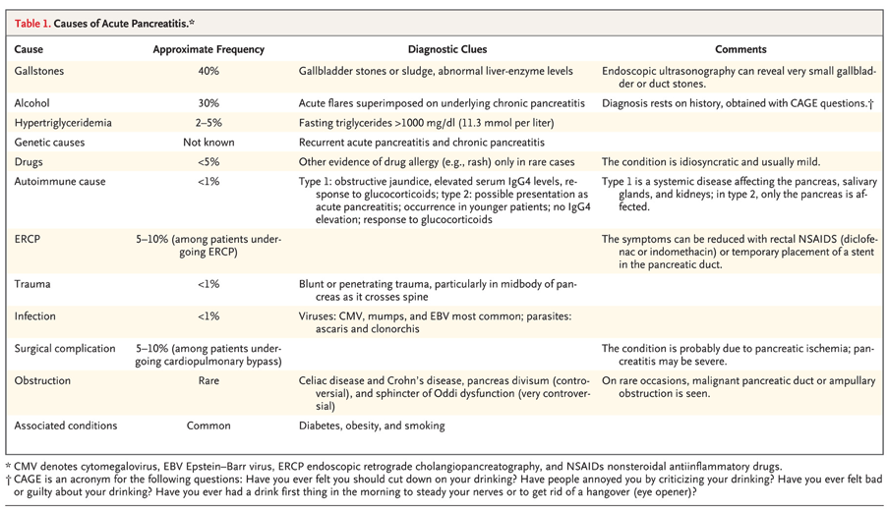
- Gallstones
- 40-70% of cases
- Only 3-7% of patients with gallstones develop pancreatitis
- Two theorized mechanisms
- Reflux of bile into the pancreatic duct
- Obstruction at the ampulla
- Magic number is 5mm
- Small enough to pass through cystic duct, but still get obstructed at ampulla
- 40-70% of cases
- Alcohol
- 25-35% of cases
- Interesting data to show that it is not just alcohol that causes pancreatitis
- 5 out of 100,00 patents with alcohol abuse develop pancreatitis
- Several mechanisms theorized
- Sensitization of acinar cell to CCK-induced activation of zymogens
- Potentiation of the effect of CCK
- Generation of toxic metabolites
- Sensitization of the pancreas to toxic insults
- Activation of pancreatic stellate cells to increase production of matrix proteins
- Idiopathic (genetic)
- 15-25% of patients with pancreatitis have no identifiable pathologic cause
- These cases are largely theorized to have complex genetic risk profiles
- Hypertriglyceridemia
- 1-14% of cases
- > 1000 mg/dL increases risk
- Post-ERCP
- 3% of patients undergoing diagnostic ERCP
- 5% of patients undergoing therapeutic ERCP
- 25% of patients undergoing sphincter of Oddi measurements
- Medications
- < 5% of cases
- Classification system (Ia, Ib, II, III, IV)
- Prognosis is excellent and mortality is very low
- Obesity
- Smoking
- Diabetes

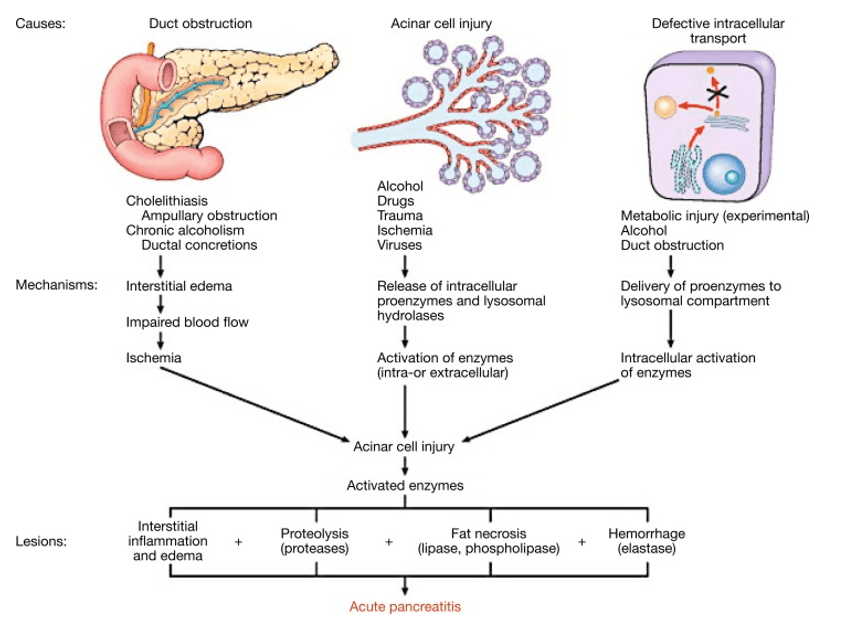
Pathogenesis
- Pancreatic enzymes synthesis continues while secretion is slowed or halted
- HIT #1 – Intraacinar activation of proteolytic enzymes (trypsin)
- Cascade of enzyme release and activation then occurs
- Ultimately, causes autodigestion of the pancreas
- HIT #2 – Microcirculatory injury
- Damage to the pancreas via autodigestion leads to vasoconstriction, decreased oxygenation, and progressive ischemia
- Leads to edema and further decreased secretion of enzymes
- Damage to the pancreas via autodigestion leads to vasoconstriction, decreased oxygenation, and progressive ischemia
- HIT #3 – Leukocyte infiltration, cytokine release, and oxidative stress
- Leads to widespread inflammation and induce thrombosis and hemorrhage
- Ultimately, causes necrosis
- Two main classifications
- Interstitial pancreatitis – blood supply is maintained
- Necrotizing pancreatitis – blood supply is affected
Signs and Symptoms
- History
- Epigastric pain
- May radiate to the back
- May radiate to the right shoulder
- Kehr’s sign
- Nausea
- Vomiting
- Dyspneic
- Severe disease can cause diaphragmatic irritation and pleural effusions
- Epigastric pain
- Physical Examination
- Fever
- Tachycardia
- Epigastric tenderness
- Abdominal distention
- Hypoactive bowel sounds
- Jaundiced
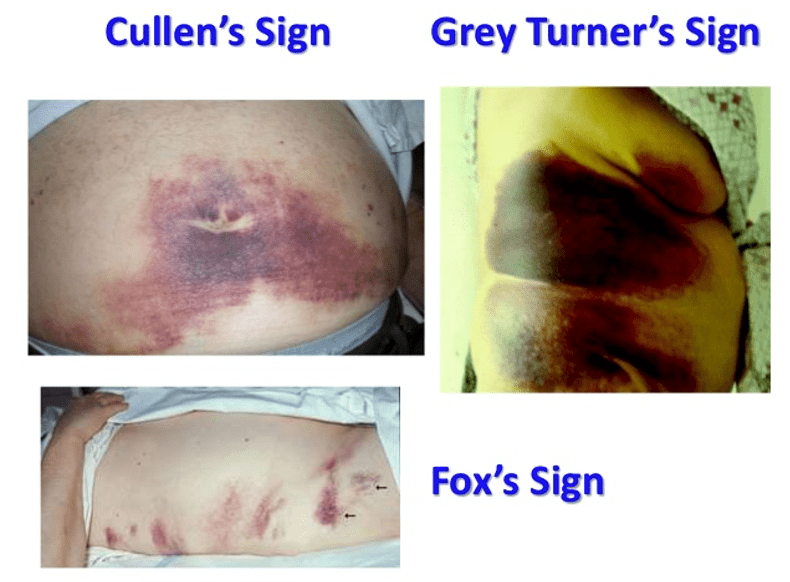
- Abdominal ecchymosis (necrotizing disease)
- Cullen’ sign – umbilical
- Grey Turner’s sign – flank
- Fox’s sign – thigh (parallel but inferior to inguinal ligament)
Laboratory Studies
- Serum amylase
- Rises within 6 hours, returns to normal in 3-5 days
- Should not be used (sensitivity 67-83%, specificity 85-98%)
- Short-half life (10 hours)
- Patients presenting > 24 hours after onset can have normal amylase
- Miss up to 20% of cases of alcohol pancreatitis
- Due to inability of parenchyma to produce amylase
- Miss up to 50% of cases of hypertriglyceridemia
- Triglycerides interfere with assay
- Short-half life (10 hours)
- Serum lipase
- Sensitivity 85-100%
- Rises 4-8 hours, peaks at 24 hours, returns to normal in 8-14 days
- LFTs
- Evaluate for cholestatic elevations (ALP, bilirubin, GGT)
- BMP
- Need glucose, BUN, and calcium for some of the risk calculators
- CBC
- Leukocytosis often is present and helps grade severity
- May show hemoconcentration due to volume depletion
Imaging Studies
- Ultrasound
- Often the quickest and easiest study to obtain in the ED
- Can evaluate gallbladder pathology, stones, and peripancreatic fluid
- Ileus can obscure imaging due to gas overlying the pancreas
- CT
- Better detail and can evaluate more structures

- MRI
- Higher sensitivity in early disease
- Longer to obtain
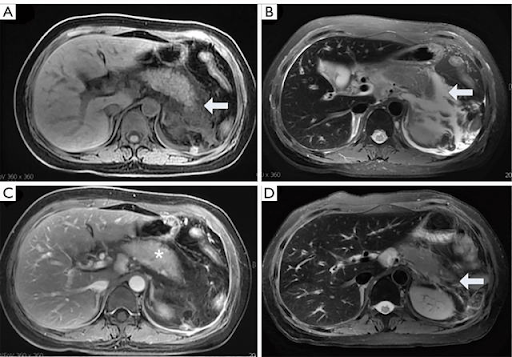
- Revised Atlanta Criteria
- Six CT morphological features
- Interstitial edema
- Parenchymal enhancement by IV contrast
- Necrotizing findings
- Lack of parenchymal enhancement
- Peripancreatic fluid collection or walled-off necrosis
- Acute peripancreatic fluid collection
- Homogenous fluid collection
- Confined to normal peripancreatic fascial planes
- No definable encapsulating wall
- Adjacent to pancreas (no intrapancreatic extension)
- Pancreatic pseudocyst
- Well-circumscribed, well-defined wall with homogenous fluid density
- No non-liquid component
- Acute necrotic collection
- Heterogenous with non-liquid density of varying degrees
- No definable wall
- Intra-, or extra-pancreatic in location
- Walled-off necrosis
- Heterogenous with liquid and non-liquid densities
- Well-defined wall that is completely encapsulated
- Intra-, or extra-pancreatic in location
Diagnosis
- Need 2 of the following 3 criteria:
- Acute onset of persistent, severe, epigastric pain
- Elevation of amylase or lipase > 3x ULN
- Radiographic findings on imaging
Classification of Severity
- Mild
- Absence of organ failure or local/systemic complications
- Moderately severe
- Transient organ failure (resolves with 48 hours) and/or systemic complications without persistent organ failure
- Severe
- Persistent organ failure

Prognosis Predictor Scoring Systems
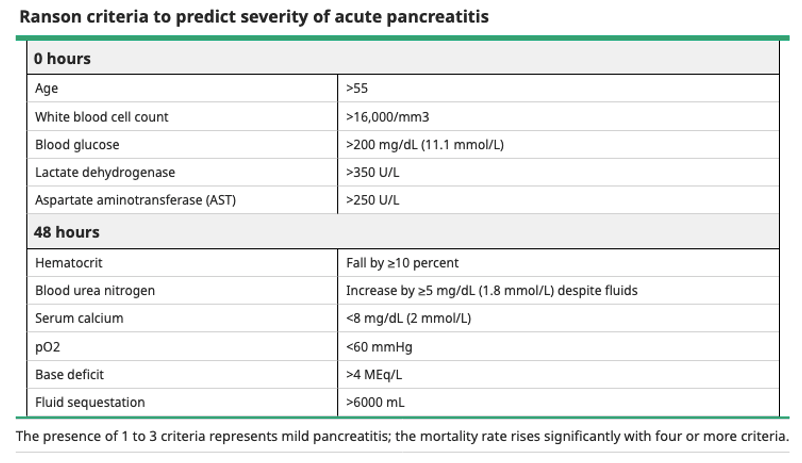
- Ranson’s Criteria
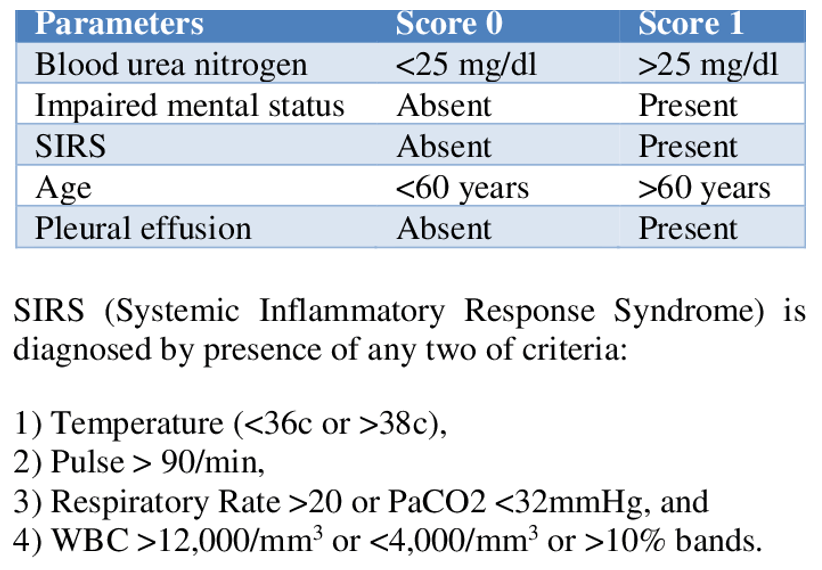
- BISAP Score
- 0-2 points – low mortality
- 3-5 points – high mortality
Management
- Patients with mild pancreatitis can be admitted to floor/wards
- Patients with moderately severe or severe should be admitted to ICU
- Fluid resuscitation
- 5-10 mL/kg/hour with crystalloid
- Careful, using LR in patients with hypercalcemic induced pancreatitis
- Bolus 20 ml/kg over 30 minutes if hypotensive/tachycardic
- Adjust using goal-directed metrics even 6 hours for first 24 hours-48 hours
- BUN, H/H, MAP (65-85 mmHg), HR (< 120bpm), UOP (>0.5 mL/kg/hr)
- 5-10 mL/kg/hour with crystalloid
- Pain control
- Opioids are safe and PCA can work well
- Fentanyl has better safety profile
- 20-50 mcg with 10-min lockout
- Fentanyl has better safety profile
- Opioids are safe and PCA can work well
- Nutrition
- Can reintroduce within 24 hours if no nausea, vomiting, and decreasing pain and inflammatory markers
- Start with low-residue, low fat, soft diet and advance as tolerated
- Supplemental nutrition generally needed for moderately severe and severe cases, or if unable to tolerate oral nutrition within 5 days
- Enteral > parental with placement of jejunal feeding tube beyond the ligament of Treitz
- Helps prevent bacterial translocation
- Parenteral is indicated if nutritional goals are not achieved with 48-72 hours due to pain or intolerance
- Consult your hospital nutritional team and/or dietician for help
- Enteral > parental with placement of jejunal feeding tube beyond the ligament of Treitz
- Can reintroduce within 24 hours if no nausea, vomiting, and decreasing pain and inflammatory markers
- Antibiotics
- No evidence to support prophylactic antibiotics
- Most infected necroses will occur late in clinical course (5-10 days after admission)
- No evidence to support prophylactic antibiotics
- Treat underlying causes
- Gallstone pancreatitis
- ERCP should be performed within 24 hours of admission
- Cholecystectomy should be performed within 7 days and often during same hospitalization
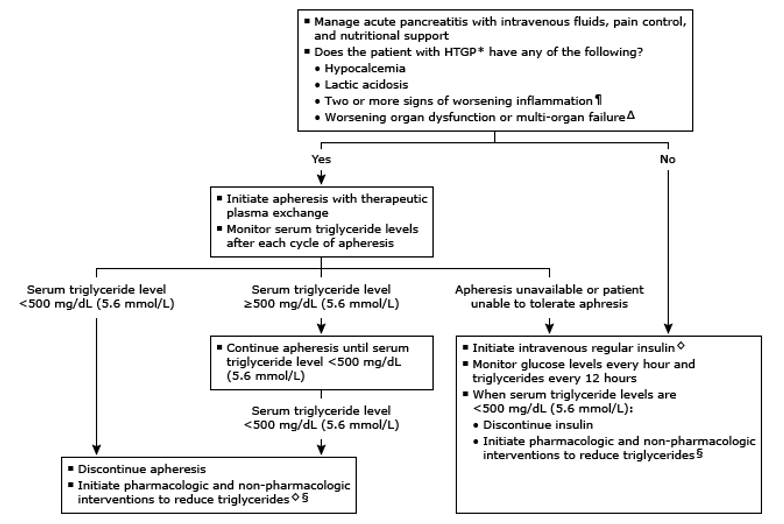
- Hypertriglyceridemia
- Therapeutic plasma exchange and insulin therapy
- Gallstone pancreatitis
Complications
- Necrosis
- Pseudocyst
- Splanchnic venous thrombosis
References
- Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013; 144(6):1252-61. [PDF]
- Conwell DL, Banks PA, Greenberger NJ. Acute and Chronic Pancreatitis. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e. McGraw-Hill;
- Mechanisms of alcoholic pancreatitis. Proceedings of a conference. Chicago, Illinois, USA, November 2002. Pancreas. 2003; 27(4):281-355. [pubmed]
- Nawaz H, Koutroumpakis E, Easler J, et al. Elevated serum triglycerides are independently associated with persistent organ failure in acute pancreatitis. Am J Gastroenterol. 2015; 110(10):1497-503. [pubmed]
- Scherer J, Singh VP, Pitchumoni CS, Yadav D. Issues in hypertriglyceridemic pancreatitis: an update. J Clin Gastroenterol. 2014; 48(3):195-203. [PDF]
- Kahaleh M, Freeman M. Prevention and management of post-endoscopic retrograde cholangiopancreatography complications. Clin Endosc. 2012; 45(3):305-12. [PDF]
- Lankisch PG, Dröge M, Gottesleben F. Drug induced acute pancreatitis: incidence and severity. Gut. 1995; 37(4):565-7. [PDF]
- Forsmark CE, Swaroop Vege S, Wilcox CM. Acute Pancreatitis N Engl J Med. 2016; 375(20):1972-1981.
- Yadav D, Agarwal N, Pitchumoni CS. A critical evaluation of laboratory tests in acute pancreatitis. Am J Gastroenterol. 2002; 97(6):1309-18. [pubmed]
- Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, Banks PA. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut. 2008; 57(12):1698-703. [pubmed]
- Vege SS, DiMagno MJ, Forsmark CE, Martel M, Barkun AN. Initial Medical Treatment of Acute Pancreatitis: American Gastroenterological Association Institute Technical Review. Gastroenterology. 2018; 154(4):1103-1139. [pubmed]
- Basurto Ona X, Rigau Comas D, Urrútia G. Opioids for acute pancreatitis pain. Cochrane Database Syst Rev. 2013; [pubmed]
- Casaer MP, Mesotten D, Hermans G, et al. Early versus late parenteral nutrition in critically ill adults. N Engl J Med. 2011; 365(6):506-17. [pubmed]
- Kutsogiannis J, Alberda C, Gramlich L, et al. Early use of supplemental parenteral nutrition in critically ill patients: results of an international multicenter observational study. Crit Care Med. 2011; 39(12):2691-9. [pubmed]
- Aboulian A, Chan T, Yaghoubian A, et al. Early cholecystectomy safely decreases hospital stay in patients with mild gallstone pancreatitis: a randomized prospective study. Ann Surg. 2010; 251(4):615-9. [pubmed]
- Uhl W, Müller CA, Krähenbühl L, Schmid SW, Schölzel S, Büchler MW. Acute gallstone pancreatitis: timing of laparoscopic cholecystectomy in mild and severe disease. Surg Endosc. 1999; 13(11):1070-6. [pubmed]
- Ipe TS, Pham HP, Williams LA 3rd. Critical updates in the 7 edition of the American Society for Apheresis guidelines. J Clin Apher. 2018; 33(1):78-94. [pubmed]
