

***LISTEN TO THE PODCAST HERE***
DEFINITION
- Acute monophasic paralyzing illness usually provoked by a preceding event
- Most commonly this is an infection (2/3rds of patients)
- Other causes
- Immunizations
- Influenza, meningococcal (MCV4)
- Surgery
- Trauma
- Medications
- Immunizations
- Was considered to be a SINGLE condition, but now is recognized to be an umbrella term for a mix of many different variants
- Acute inflammatory demyelinating polyradiculoneuropathy (AIDP)
- Most common in the US (85-90%)
- Miller Fisher syndrome (MFS)
- Acute motor axonal neuropathy (AMAN)
- Acute sensorimotor axonal neuropathy (AMSAN)
- Acute inflammatory demyelinating polyradiculoneuropathy (AIDP)

EPIDEMIOLOGY
- 1-2 cases per 100,000 per year
- Incidence increases 20% with every 10-year increase in age after the first decade of life
- Slightly higher incidence in men than women

PATHOGENSIS
- Molecular Mimicry
- Antecedent event provokes an immune response, which produces antibodies that cross-reacts with nerve components due to the sharing of epitopes
- If directed at Schwann cell surface membranes à AIDP
- Infiltration of lymphocytes in the epineural and endoneural veins causing myelin degeneration at the dorsal and ventral roots
- If directed at axonal membrane à AMAN and AMSAN
- Attack is directed at the nodes of Ranvier of the ventral roots of the peripheral nerves
- If directed at Schwann cell surface membranes à AIDP
- End result is blocking the neuro-electrical transmission of impulses
- Antecedent event provokes an immune response, which produces antibodies that cross-reacts with nerve components due to the sharing of epitopes
- Common infections
- C. jejuni (most common)
- HIV
- H. influenza
- M. pneumoniae
- CMV




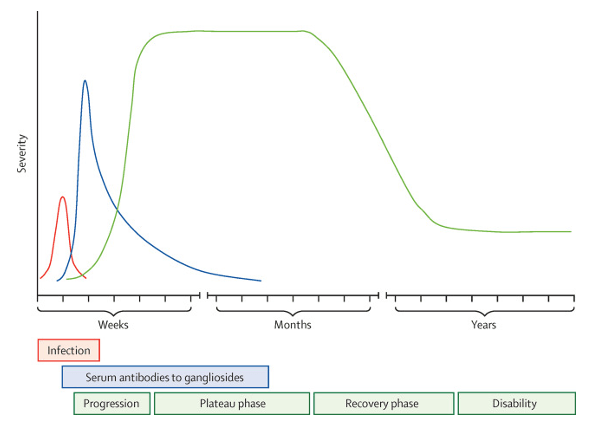
CLINICAL FEATURES
- Ascending (distal to proximal) symmetric muscle weakness with absent deep tendon reflexes progressing over days to weeks
- Weakness can vary from mild difficulty with walking to complete paralysis
- Symptom peak at around 4 weeks
- Respiratory dysfunction – 10-30%
- Facial nerve palsies or oropharyngeal weakness – 50%
- Oculomotor – 15%
- Paresthesias – 80%
- Dysautonomia – 70%
- Diarrhea, constipation, hyponatremia, bradycardia, urinary retention
- Variant Discrepancies
- AMAN – preservation of deep tendon reflexes
- AMSAN – more sensory disturbances
- Miller Fisher – ophthalmoplegia with ataxia and areflexia
DIAGNOSIS
- CSF Analysis
- Albuminocytologic dissociation
- Elevated protein with normal WBC
- Present within first week and peaks at 3 weeks
- Thought to be due to the increased permeability of the blood-nerve-barrier of the proximal roots
- Albuminocytologic dissociation
- Electrodiagnostic Studies (EMG and NCS)
- Demyelinating forms
- Decreased motor nerve conduction velocity
- Prolonged distal motor latency
- Complete conduction blocks
- Axonal forms
- Decreased distal motor and/or sensory amplitudes
- Serial studies can be helpful since the condition can progress over time
- Demyelinating forms
- Antibodies
- Specific autoantibodies can help differentiate variant subtypes
- MRI
- Thickening and enhancement of the intrathecal spinal nerve roots and cauda equina

DIAGNOSTIC CRITERIA
- Developed in 1978 and modified over the decades based on evolving research

TREATMENT
- Supportive care
- Respiratory support
- Up to 30% will require ventilatory support
- Impending respiratory arrest
- FVC < 20 mL/kg
- Maximum inspiratory pressure < 30 cmH2O
- Maximum expiratory pressure < 40 cmH2O
- Predictors of respiratory failure
- Time of onset to admission < 7 days
- Inability to cough, stand, lift elbows, or lift head
- Elevated LFTs
- Vital capacity < 60% predicted
- Online tool to help predict
- Autonomic Dysfunction
- Cardiovascular monitoring and support
- Hypertension and hypotension
- Bradycardia and tachydysrhythmias
- Bowel and Bladder care
- Urinary retention
- Ileus management
- Cardiovascular monitoring and support
- Respiratory support
- Disease-Modifying Treatment
- Started within 4 weeks of symptom onset
- Plasma exchange
- Remove circulating autoantibodies
- 4-6 treatments over 8-10 days
- Complications
- Hypotension, sepsis
- IVIG
- Interferes with production and function of cytokines, B-cells, and T-cells
- 0.4 grams/kg/day for 5 days
- Complications
- Meningitis, rash, renal failure

PROGNOSIS
- 60% will fully recover by 1 year
- 15% will have persistent severe motor problems
- 3-7% will succumb to the illness
- 20% of patients requiring mechanical ventilation
COTTAGE PHYSICIAN (1893)

REFERENCES
- Gibbons CH, Engstrom JW. Disorders of the Autonomic Nervous System. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e. McGraw-Hill; Accessed May 09, 2021.
- Diseases of the Peripheral Nerves. In: Ropper AH, Samuels MA, Klein JP, Prasad S. eds. Adams and Victor’s Principles of Neurology, 11e. McGraw-Hill; Accessed May 09, 2021.
- Yuki N, Hartung HP. Guillain-Barré syndrome. N Engl J Med. 2012; 366(24):2294-304. [pubmed]
- Willison HJ, Jacobs BC, van Doorn PA. Guillain-Barré syndrome. Lancet. 2016; 388(10045):717-27. [pubmed]
- Sejvar JJ, Baughman AL, Wise M, Morgan OW. Population incidence of Guillain-Barré syndrome: a systematic review and meta-analysis. Neuroepidemiology. 2011; 36(2):123-33. [PDF]
- Alshekhlee A, Hussain Z, Sultan B, Katirji B. Guillain-Barré syndrome: incidence and mortality rates in US hospitals. Neurology. 2008; 70(18):1608-13. [pubmed]
- Fokke C, van den Berg B, Drenthen J, Walgaard C, van Doorn PA, Jacobs BC. Diagnosis of Guillain-Barré syndrome and validation of Brighton criteria. Brain. 2014; 137(Pt 1):33-43. [pubmed]
- Hadden RD, Cornblath DR, Hughes RA, et al. Electrophysiological classification of Guillain-Barré syndrome: clinical associations and outcome. Plasma Exchange/Sandoglobulin Guillain-Barré Syndrome Trial Group. Ann Neurol. 1998; 44(5):780-8. [pubmed]
- Lawn ND, Fletcher DD, Henderson RD, Wolter TD, Wijdicks EF. Anticipating mechanical ventilation in Guillain-Barré syndrome. Arch Neurol. 2001; 58(6):893-8. [pubmed]
- Raphaël JC, Chevret S, Hughes RA, Annane D. Plasma exchange for Guillain-Barré syndrome. Cochrane Database Syst Rev. 2012; [pubmed]
- Hughes RA, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barré syndrome. Cochrane Database Syst Rev. 2014; [PDF]
