
***LISTEN TO THE PODCAST HERE***
Epidemiology
- Comprise 15% of all CHD and 33% of potentially fatal CHD
Physiology
The cardiovascular system in-utero is a complicated machine that is designed to bypass the lungs and provide oxygenated blood from the placenta. There are two main structures that help maintain oxygenation when the fetus’ lungs are not used:
- Ductus arteriosus
- Connects the pulmonary artery to the descending aorta
- Prostaglandin E1 and E2 are produced by the placenta and keep this open
- Absolutely vital to remain patent in several of the cyanotic diseases to provide oxygenated blood
- Foramen ovale
- Communication between right and left atrium
- Once the infant begins spontaneously breathing, increases in pulmonary blood flow and left atrial pressures mechanically seals the foramen ovale
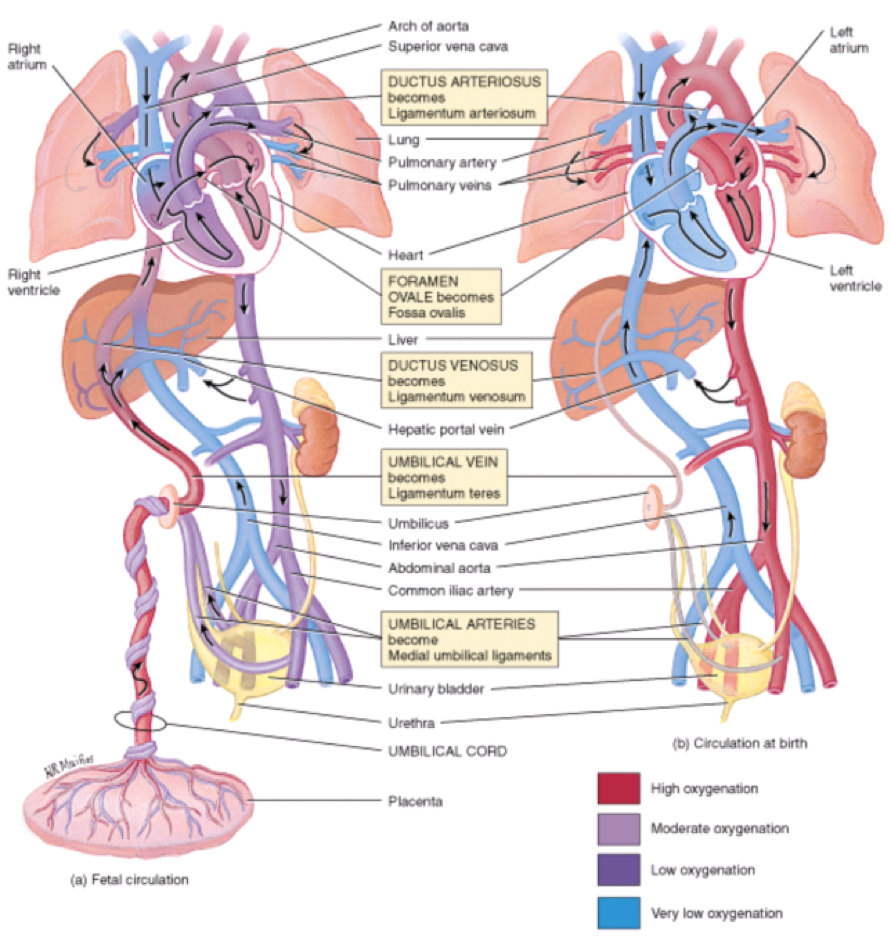
Fetal circulation (a) in-utero and (b) during 1st 7 days of life
Khan Academy Tutorials
Cardiac Causes of Cyanosis
- 3 Main Physiologic Categories
- Decreased pulmonary blood flow
- Tetralogy of Fallot, tricuspid atresia
- Increased pulmonary blood flow
- Transposition of great vessels, truncus arteriosis, total anomalous pulmonary venous connection
- Severe heart failure
- Hypoplastic left heart, coarctation of the aorta
- Decreased pulmonary blood flow
Timing of Presentation
- Within 48 hours of birth
- Transposition of great vessels, tricuspid atresia
- With 7 days of birth
- Truncus arteriosus, total anomalous pulmonary venous connection, Tetralogy of Fallot
Screening
- Hyperoxia Test
- 100% oxygen via hood for 10 minutes
- Radial artery (preductal) PaO2 is measured
- PaO2 > 150 mmHg suggests pulmonary disease
- Pulse Oximetry Screening
- Measuring the difference in SpO2 between preductal (right hand) and postductal (either foot) flow
- A positive test warranting further investigation includes any of the following:
- SpO2 < 90% in either extremity
- SpO2 90-94% in both locations on three measurements one hour apart
- SpO2 difference > 3% on three measurements one hour apart

Pulse Oximetry Screening Test http://www.cdc.gov/ncbddd/heartdefects/hcp.html
Work-Up
- Physical exam findings
- Murmur
- Second heart sound (normally split in inspiration)
- Chest radiograph
- Differentiates pulmonary from cardiac causes of cyanosis
- Heart size often increased with some classic shapes
- Electrocardiogram
- Normal neonatal EKG has RAD
- Hypertrophy and enlargement specific to defects
- All cyanotic defects are diagnosed by echocardiogram and/or cardiac angiography
Tetralogy of Fallot

- Most common cyanotic congenital heart defect
- 1st described in 1888 by Etienne-Louis Arthur Fallot
- 4 key features
- Pulmonary stenosis
- Overriding aorta
- VSD
- Right ventricular hypertrophy
- Signs and Symptoms
- Cyanosis can be seen at birth, but usually presents by 4 months
- Palpable RV lift
- Single, aortic S2
- Systolic murmur at left sternal border in 3rd intercostal space
- Chest radiograph may show “boot shaped heart” and right aortic knob
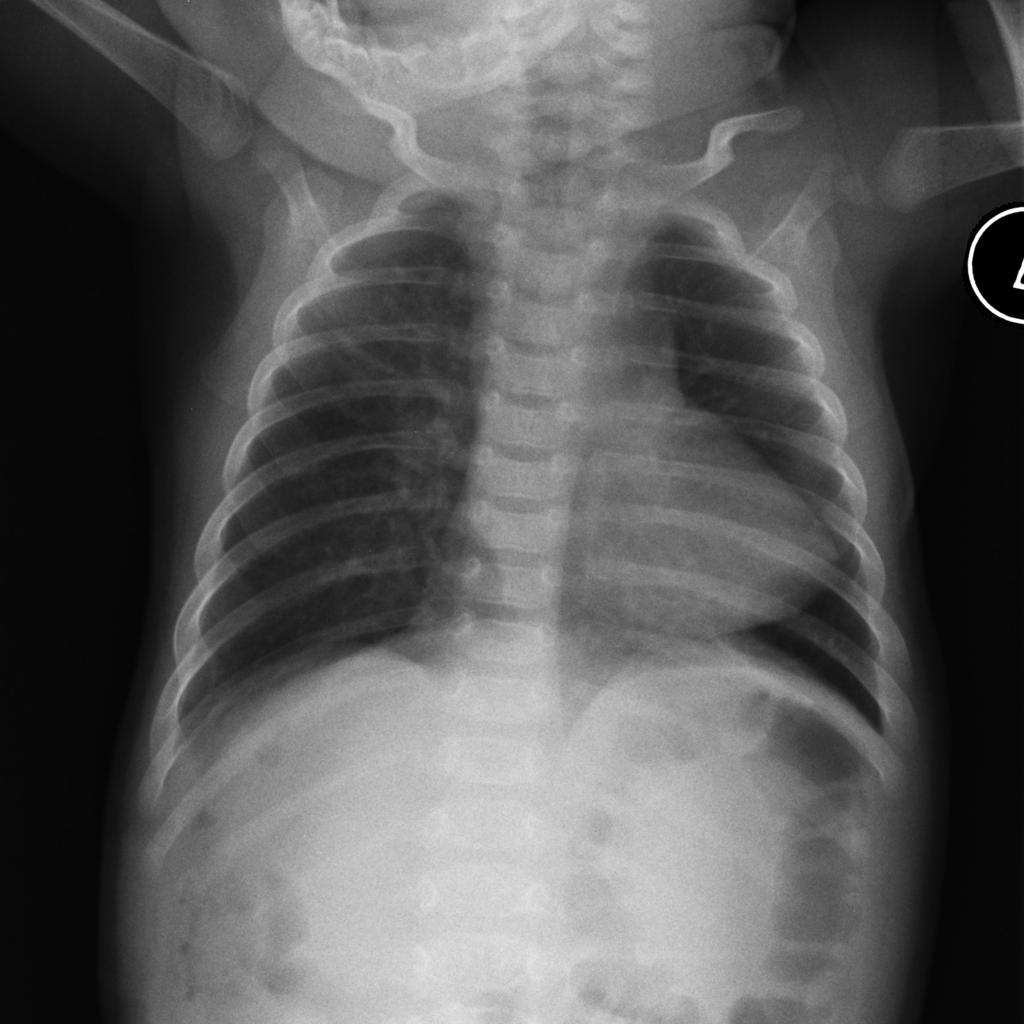
“boot shaped heart” Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org. From the case rID: 8049
- “Tet spells”
- Near complete right ventricular outflow obstruction resulting in:
- Sudden onset or worsening of cyanosis
- Dyspnea
- Alterations in consciousness or irritability
- Decrease or disappearance of murmur
- Causes
- Agitation in infants
- Vigorous exercise in older children
- Often self correct by squatting down and bringing knees to chest in increases pulmonary blood flow
- Near complete right ventricular outflow obstruction resulting in:
- Surgical repair is performed anytime from birth to 2 years depending on size of pulmonary arteries

D-Transposition of Great Vessels

- 2nd most common cyanotic defect
- Embryologic ventriculoarterial discordance (2 parallel circuits)
- Aorta is anterior and comes off right ventricle
- Pulmonary artery comes off left ventricle
- VSD are common and ASD/PFO is critical for survival to allow mixing
- Signs and Symptoms
- Generally present within 1st month of life
- Tachypnic, but comfortable without signs of respiratory distress
- Pansystolic murmur of VSD
- Chest radiograph may show classic “egg of a string”

“egg on a string sign” Case courtesy of Dr David Clopton, Radiopaedia.org. From the case rID: 35346
- EKG is non-diagnostic
- Surgical repair is performed at 7 days
- Arterial Switch Operation
- 95% survival
- Arterial Switch Operation
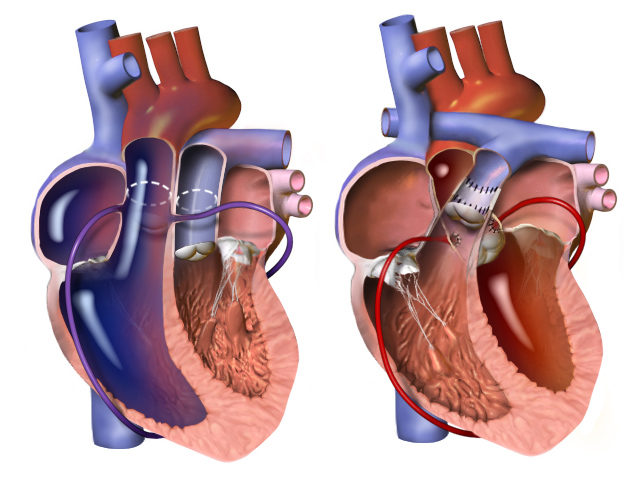
Arterial Switch Operation https://en.wikipedia.org/wiki/Jatene_procedure
Tricuspid atresia
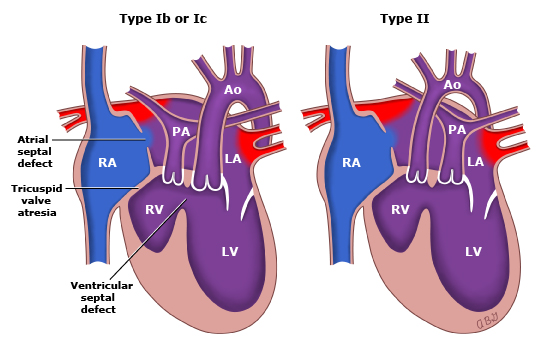
- 3rd most common cyanotic defect
- Complete absence of tricuspid valve and no direct communication between right atrium and ventricle
- ASD and PFO allow right-to-left flow
- Right ventricular hypoplasia depending on VSD size
- 3 types
- Type I
- Ia – normal great vessel anatomy with no VSD
- PDA is sole source of pulmonary blood flow
- Ib and Ic– normal great vessel anatomy with a VSD
- Ia – normal great vessel anatomy with no VSD
- Type II
- Transposition of great vessels with VSD
- Type I
- Signs and Symptoms
- Prenatal
- Can be diagnosed by fetal ultrasound between 18 and 22 weeks
- Postnatal
- Cyanosis usually in first 24 hours, but may be as late as 1 month
- Single S2 heart sound
- Holosystolic murmur over left sternal border with diastolic rumble
- Prenatal
- Chest radiograph may show smooth convexity of right heart with cardiomegaly
- Electrocardiogram may show tall P waves, LAD, LVH, and RAE
- Surgical repair performed in 3 stages
- 1st stage performed immediately
- Ensures pulmonary blood flow and unobstructed flow from LV, and protect pulmonary artery bed
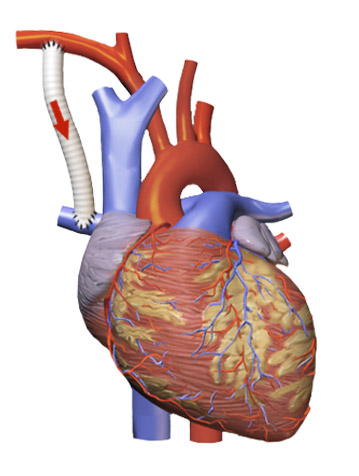
- Modified Blalock-Taussig shunt
- Innominate to pulmonary artery

Modified Blalock-Taussig Shunt https://en.wikipedia.org/wiki/Blalock%E2%80%93Taussig_shunt
- Innominate to pulmonary artery
- Modified Blalock-Taussig shunt
- Ensures pulmonary blood flow and unobstructed flow from LV, and protect pulmonary artery bed
- 2nd stage at 3-6 months
- Glenn procedure
- Take down shunt
- Cavopulmonary anastomosis to ensure passive venous drainage from SVC into pulmonary artery
- Glenn procedure
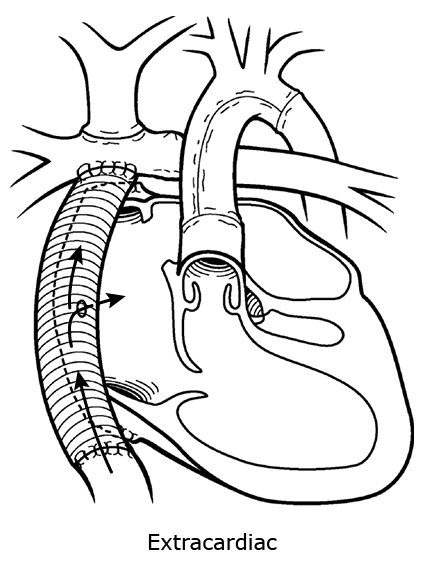
- 3rd stage at 2-3 years
- Fontan procedure
- Direct anastomosis of pulmonary arteries to right atrium
- Fontan procedure
- 1st stage performed immediately


Fontan Procedure for tricuspid atresia https://en.wikipedia.org/wiki/Fontan_procedure
Truncus Arteriosus

- Embryological failure of the division of the common truncus arteriosus into the aorta and pulmonary artery
- Single common arterial trunk positioned above the ventricular septum that gives rise to the systemic, pulmonary, and coronary circulation
- There is a single semilunar valve
- VSD is always present
- 2 main classification systems (based on pulmonary circulation anatomy)
- Collet and Edwards (1st and most simple)
- Modified Van Praagh (mainly used by pediatric cardiac surgeons)
- Signs and Symptoms
- Mild to moderate cyanosis
- Heart failure is common
- Hyperactive precordium with systolic thrill at left sternal border
- Early systolic ejection click
- Accentuated, single S2
- Diastolic flow murmur over apex
- Chest radiography may show cardiomegaly with increased pulmonary markings and right sided aortic arch
- Electrocardiography is non-diagnostic
- Surgical repair must be performed in neonatal period due to increased risk of pulmonary vascular disease and progressive, irreversible heart failure
- 3 main steps
- Pulmonary arteries are mobilized and reattached via pulmonary artery conduit to the right ventricle
- Opening and repair of the truncus
- Closure of VSD
- 3 main steps

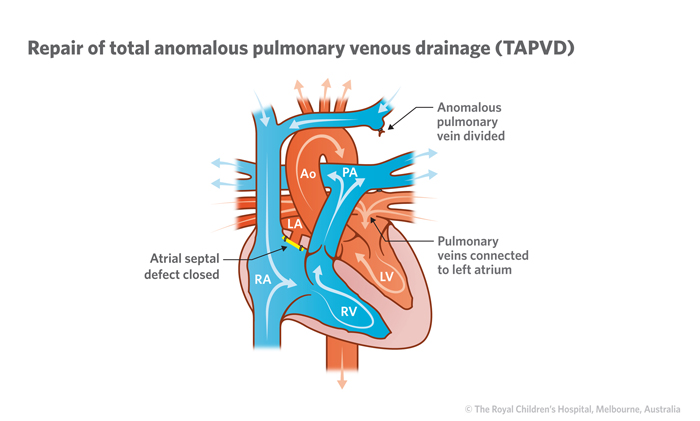
Total Anomalous Pulmonary Venous Connection
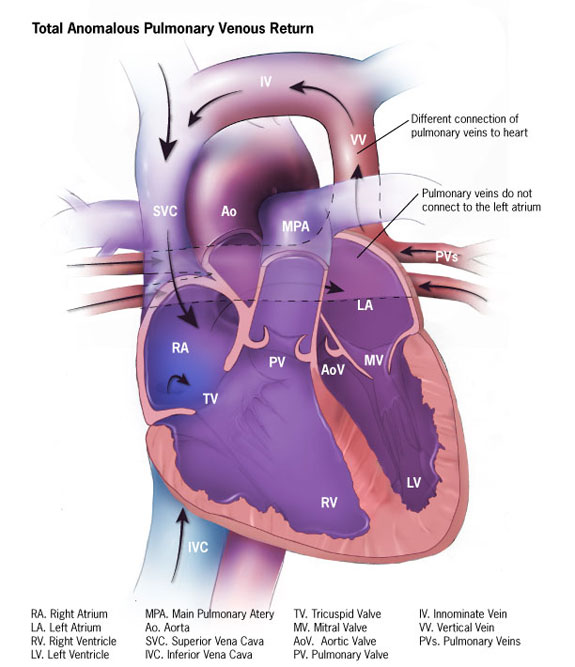
- All four pulmonary veins draining into a confluence behind the left atrium
- No connection into the left atrium and drains into systemic circulation
- 4 obstructive types
- Supracardiac (most common)
- Drains into the right SVC, left SVC, or innominate vein
- Intracardiac
- Drains into coronary sinus
- Infracardiac
- Drains into portal venous system
- Mixed
- Supracardiac (most common)
- Entire venous drainage (systemic and pulmonary) goes into right atrium
- Must have a ASD or PFO
- Signs and Symptoms
- Unobstructive
- Mild cyanosis, tachypnea
- RV heave
- Fixed split S2
- Systolic ejection murmur with diastolic rumble
- Obstructive
- Severe cyanosis and respiratory distress
- Striking RV impulse
- Accentuated, single S2
- Murmur is often absent
- Unobstructive
- Chest radiography
- Unobstructive – cardiomegaly with increased pulmonary markings, “snowman sign”
- Obstructive – small heart
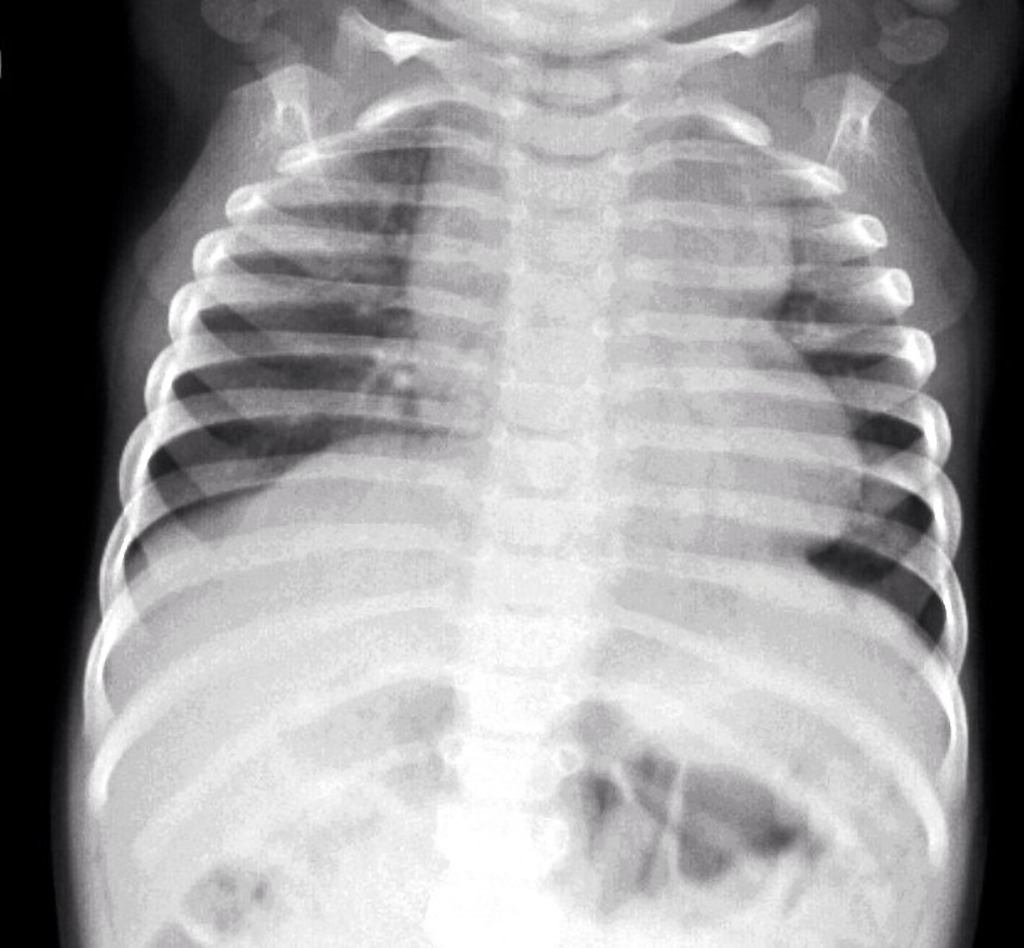
“snowman sign” Case courtesy of Dr Aditya Shetty, Radiopaedia.org. From the case rID: 27800
- Electrocardiography may show RAD, RAE, RVH in both types
- Surgical repair depends on type and timing depends on degree of obstruction
Hypoplastic Left Heart Syndrome
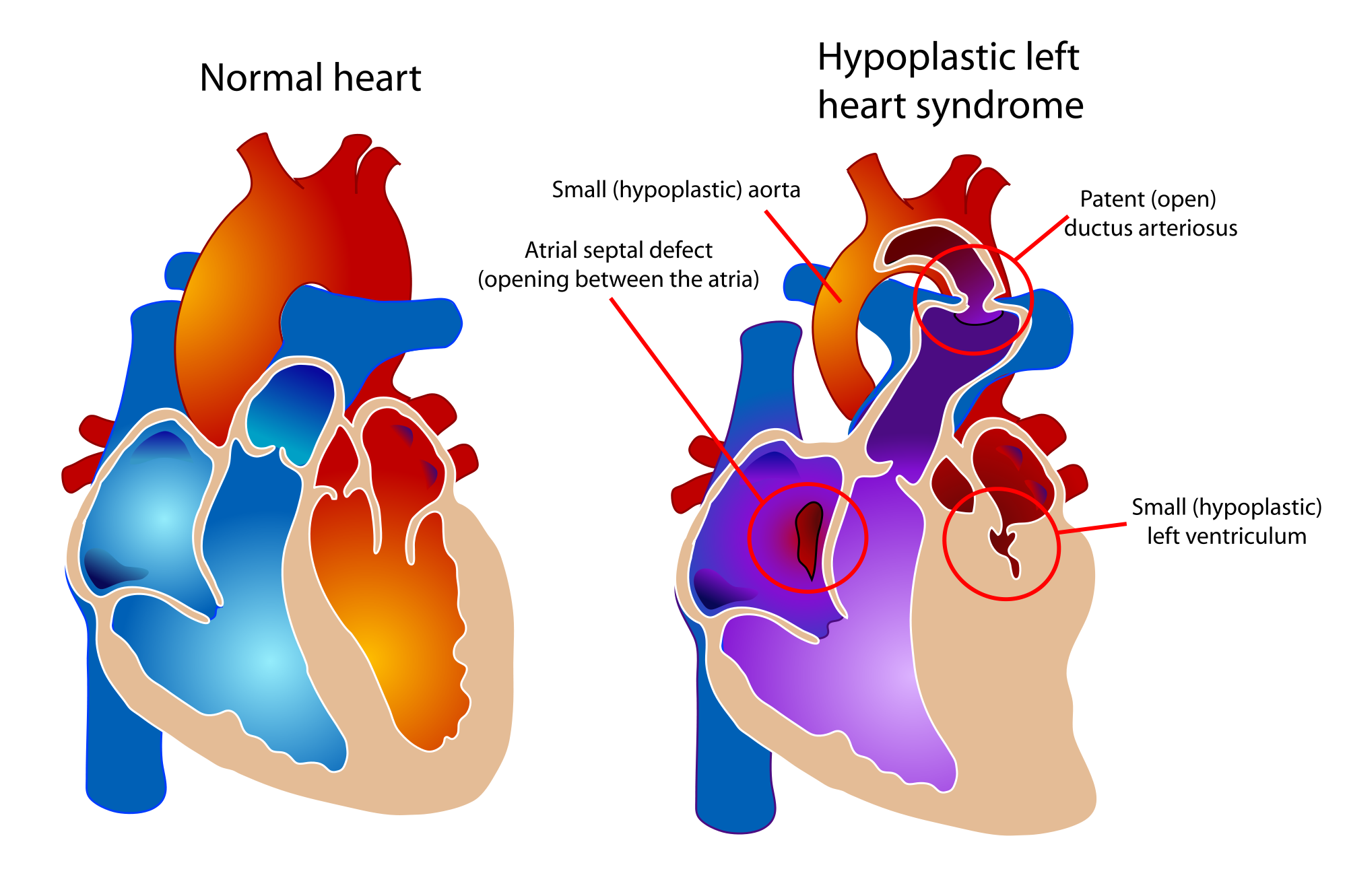
- Spectrum of cardiac malformations characterized by underdevelopment of the left ventricle with atresia, stenosis, or hypoplasia of aortic and/or mitral valve, and hypoplasia of ascending aorta and arch
- Survival is dependent on PDA and ASD
- Signs and Symptoms
- Prenatal
- Can be diagnosed by fetal ultrasound between 18-24 weeks
- Postnatal
- “Honeymoon” period while PDA is open and ASD is unrestricted
- May be discharged and present after 3-5 days
- If ASD is restricted –> rapid decompensation as PDA closes
- Single S2 heart sound
- No murmur
- “Honeymoon” period while PDA is open and ASD is unrestricted
- Prenatal
- Chest radiograph may show small cardiac silhouette
- Electrocardiogram shows RAD, RAE, RVH
- Surgical repair performed in 3 stages
- 1st stage performed immediately
- Norwood procedure (3 parts)
- Creation of neoaorta
- Blalock-Taussig shunt
- Resection of atrial septum
- Norwood procedure (3 parts)
- 1st stage performed immediately

Norwood Procedure
- 2nd stage performed at 3-6 months
- Bidirectional Glenn procedure

Bidirectional Glenn Procedure
- 3rd stage performed at 2-3 years
- Fontan procedure
- Hybrid approach and heart transplant are emerging treatment options
PAINE Pearls to Remember
6 “Ts” of Congenital Cyanotic Heart Defects
Tetralogy of Fallot
Transposition of Great Vessels
Tricuspid Atresia
Truncus Arteriosus
Total Anomalous Pulmonary Venous Connection
“Tiny” (Hypoplastic) Left Heart Syndrome
Numbers of Congenital Cyanotic Heart Defects
1 trunk (truncus arteriosus)
2 great vessels (transposition)
3 “tri” (tricuspid atresia)
4 “tetra” (Tetralogy of Fallot)
5 words (Total Anomalous Pulmonary Venous Connection)
VI – the left “I” is half as big as the right “V” (hypoplastic left heart)
Cottage Physician Reference
Nothing directly related to congenital heart defects, but I did find this quote interesting. It says:
“ The general rule as to tying the cord , with the exceptions above noticed, is, that it is the safest to delay the tying of it, until it has entirely ceased to pulsate”

The OB realm is still debating delayed cord clamping…It looks like everything in medicine always comes full circle
References
- Vetter VL, Covington TM, Dugan NP, et al. Cardiovascular deaths in children: general overview from the National Center for the Review and Prevention of Child Deaths. Am Heart J. 2015;169(3):426-437.e23.
- Wren C, Reinhardt Z, Khawaja K. Twenty-year trends in diagnosis of life-threatening neonatal cardiovascular malformations. Arch Dis Child Fetal Neonatal Ed. 2008;93(1):F33-5.
- Rudolph AM. Congenital cardiovascular malformations and the fetal circulation. Arch Dis Child Fetal Neonatal Ed. 2010;95(2):F132-6.
- Kemper AR, Mahle WT, Martin GR, et al. Strategies for implementing screening for critical congenital heart disease. Pediatrics. 2011;128(5):e1259-67.
- Marino BS, Bird GL, Wernovsky G. Diagnosis and management of the newborn with suspected congenital heart disease. Clin Perinatol. 2001;28(1):91-136.
- Darst JR, Collins KK, Miyamoto SD. Cardiovascular Diseases. In: Hay WW, Jr., Levin MJ, Deterding RR, Abzug MJ. eds. CURRENT Diagnosis & Treatment: Pediatrics, 22e. New York, NY: McGraw-Hill; 2013.
- Rao PS. Tricuspid Atresia. Curr Treat Options Cardiovasc Med. 2000;2(6):507-520.
- Tongsong T, Sittiwangkul R, Wanapirak C, Chanprapaph P. Prenatal diagnosis of isolated tricuspid valve atresia: report of 4 cases and review of the literature. J Ultrasound Med. 2004;23(7):945-50.
- Tchervenkov CI, Jacobs ML, Tahta SA. Congenital Heart Surgery Nomenclature and Database Project: hypoplastic left heart syndrome. Ann Thorac Surg. 2000;69(4 Suppl):S170-9.
- Warnes CA. Transposition of the great arteries. Circulation. 2006;114(24):2699-709.
- Lalezari S, Bruggemans EF, Blom NA, Hazekamp MG. Thirty-year experience with the arterial switch operation. Ann Thorac Surg. 2011;92(3):973-9.
- Seale AN, Uemura H, Webber SA, et al. Total anomalous pulmonary venous connection: morphology and outcome from an international population-based study. Circulation. 2010;122(25):2718-26.
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39(12):1890-900.
- Rodefeld MD, Hanley FL. Neonatal truncus arteriosus repair: surgical techniques and clinical management. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2002;5:212-7.


















{kind=link}