

Definition
The textbook definition of anemia is a reduction of the absolute number or mass of circulating red blood cells. This then causes a global reduction in the oxygen carrying capacity of the patient’s circulatory system. Clinically, we use hemoglobin and hematocrit as the surrogate markers and define anemia as 2 SD below the mean for gender:
- Men
- Hemoglobin < 13.5 g/dL
- Hematocrit < 41%
- Women
- Hemoglobin < 12.0 g/dL
- Hematocrit < 36%

Patel KV. Haematologica. 2008;93(9):1281-1283.
- Special Populations
- Athletes
- May have a baseline anemia due to:
- Dilution from increased plasma volume
- Hemolytic breakdown from exercise
- Exercise induced cytokines decreases RBC production
- A normal H/H in a competitive athlete may suggest performance enhancing drugs
- May have a baseline anemia due to:
- High altitudes
- May have elevated hemoglobin concentration as baseline
- Smokers
- Baseline higher hemoglobin due to carboxyhemoglobin
- Athletes
General Causes of Anemia
There are two general approaches you can use to help identify the cause of anemia in adults.
- The Kinetic Approach (the mechanisms responsible for the low hemoglobin)
- 3 independent mechanisms
- Decreased RBC production
- Lack of nutrients
- Bone marrow failure
- Decreased erythopoetic stimulation factors
- Erythropoietin, T3, androgens
- Inflammation
- Increased RBC destruction
- Hemolysis, hypersplenism
- Blood loss
- Decreased RBC production
- 3 independent mechanisms
- The Morphologic Approach (categories based on RBC size and reticulocyte response)
- Macrocytic (MCV > 100 fL)
- Vitamin B12, folate, EtOH, liver disease
- Any condition causing reticulocytosis
- Microcytic (MCV < 80 fL)
- 3 most common in clinical practice
- Iron deficiency
- ↓ serum iron, ↓ serum ferritin, ↑ TIBC
- Alpha or beta thalassemia minor
- Normal iron studies
- Anemia of chronic disease
- ↓ serum iron, normal serum ferritin, ↓ TIBC
- Iron deficiency
- 3 most common in clinical practice
- Macrocytic (MCV > 100 fL)
History Questions
- Is the patient symptomatic?
- Fatigue, dyspnea, bleeding, bruising, dizziness, syncope
- Any history of weight loss, night sweats, fever, anorexia?
- Infection or malignancy
- Past medical history for chronic illness
- PUD, renal disease, autoimmune conditions, liver disease, past malignancies
- Family history for hemoglobinopathies
- Social history for alcohol use
- Occupational exposures
Physical Exam Findings
- Pallor
- Palms, nail beds, face, conjunctiva
- Jaundice
- Hepatosplenomegaly
- Lymphadenopathy
- Petechiae, purpura, bruising
- Bone tenderness
Laboratory Testing
Anemia is usually first diagnosed by CBC. Once you have a documented low H/H, then you need order follow-up studies to help differentiate the cause of the anemia. These include:
- RBC indices
- MCV, MCH, MCHC, RDW
- Reticulocyte count and index
- Peripheral smear
- Helmet cells or schistocytes à microangiopathic hemolysis
- Microspherocytes à autoimmune hemolysis
- Tear drop RBC à myelofibrosis
- Bite cells à oxidative hemolysis
- Parasites à malaria, babeosis
- Hypersegmented neutrophils à Vitamin B12 or folate deficiency
- Nucleated RBC
- Siderocytes
- Target cells à thalassemias
- WBC and platelet count from CBC
- If hemolysis is suspected:
- ↑ Serum LDH, ↓ serum haptoglobin, and ↑ serum indirect bilirubin
- Direct Coombs test (antibodies against RBC)
- Bone marrow evaluation

Schrier SL, et al. Approach to adults with anemia. In: Up To Date. Waltham, MA (Accessed 03/23/2016)
The Cottage Physician Management
Something new I thought I would bring to the PAINE Podcast. As you all know, I am quite a fan of medicine and antiquity. Shortly after I married my wife, her grandfather past away from a progressive esophageal cancer. One of the things I was able to keep when helping clean out his house, was a copy of The Cottage Physician printed in 1893. It was basically a handbook on how to treat common ailments of the time. I will try to add excerpts from this book when appropriate so you can have a sense of how medicine was practiced in the late 19th century.
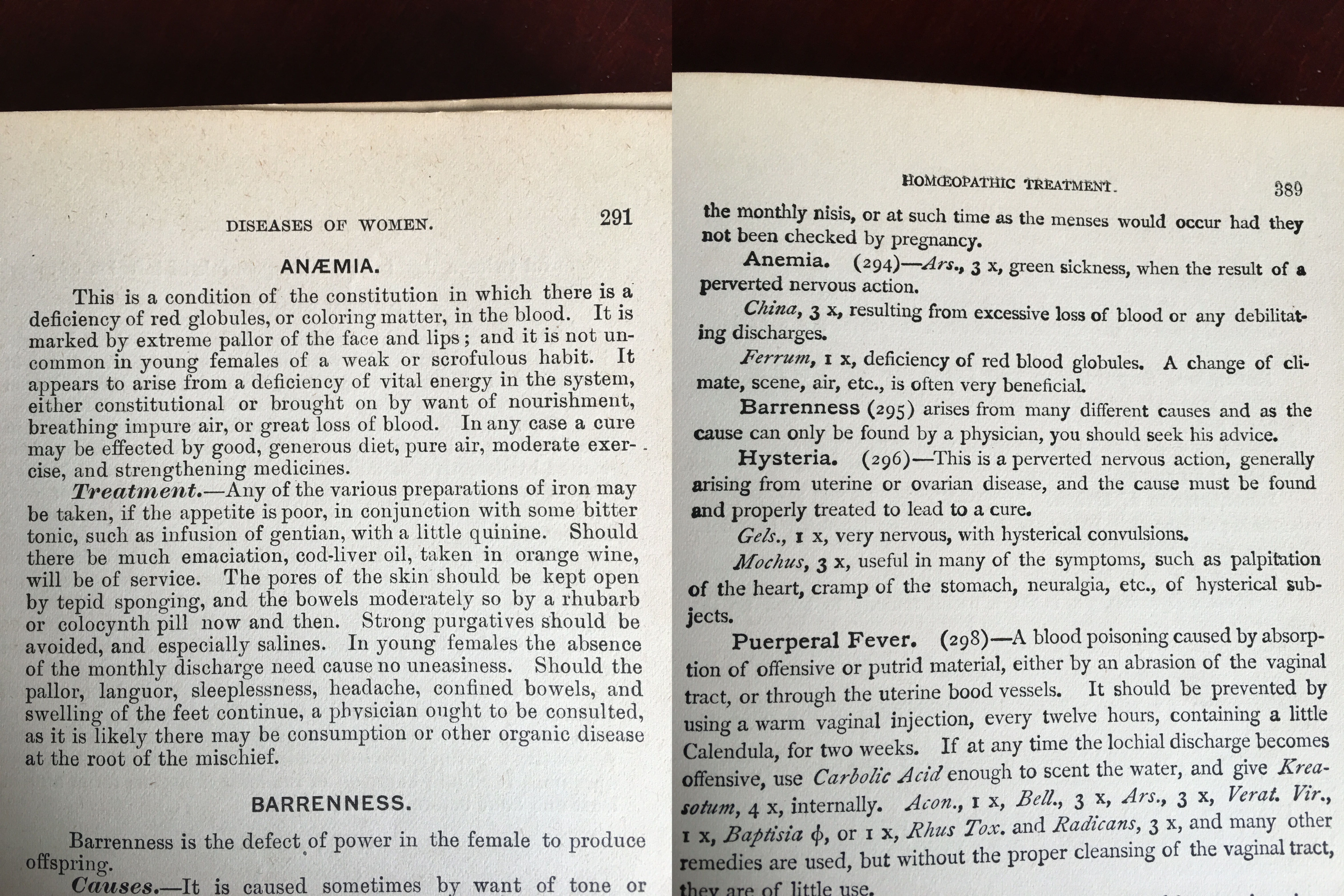
The Cottage Physician. 1863
References
- Patel KV. Variability and heritability of hemoglobin concentration: An opportunity to improve understanding of anemia in older adults. Haematologica. 2008;93(9):1281-1283.
- Beutler E, Waalen J. The definition of anemia: what is the lower limit of normal of the blood hemoglobin concentration?. Blood. 2006;107(5):1747-50.
- Shaskey DJ, Green GA. Sports haematology. Sports Med. 2000;29(1):27-38.
- Ruíz-argüelles GJ. Altitude above sea level as a variable for definition of anemia. Blood. 2006;108(6):2131.
- Nordenberg D, Yip R, Binkin NJ. The effect of cigarette smoking on hemoglobin levels and anemia screening. JAMA. 1990;264(12):1556-9.
- Hillman RS, Ault KA, Leporrier M, Rinder HM. Clinical Approach to Anemia. In: Hematology in Clinical Practice. 5th McGraw-Hill. New York. 2010.
- Tefferi A. Anemia in adults: a contemporary approach to diagnosis. Mayo Clin Proc. 2003;78(10):1274-80.
- Nardone DA, Roth KM, Mazur DJ, Mcafee JH. Usefulness of physical examination in detecting the presence or absence of anemia. Arch Intern Med. 1990;150(1):201-4.
- Hung OL, Kwon NS, Cole AE, et al. Evaluation of the physician’s ability to recognize the presence or absence of anemia, fever, and jaundice. Acad Emerg Med. 2000;7(2):146-56.
