19yo male is brought into the emergency department by EMS after getting into an altercation and getting knocked unconscious. He unsure of how long he was out, but he came to once EMS arrived. He denies any nausea, vomiting, or vision changes. He is drowsy/lethargic with his eyes closed, but is arousable to voice. He can carry on a conversation, but he needs frequent redirection and he does not know where he is. While talking with him, the nurse starts an IV and he tries to swat her away with his opposite hand.
What is the classic score we use and what is his score?
The Glasgow Coma Scale (GCS) was first devised in 1974 and has been the predominant neurologic scoring system since. It takes into account 3 main variables and each variable has a point score attached to it. The maximum score is 15 and the minimum score is 3 (3T if intubated).
- Eye opening
- 4 points – Spontaneous
- 3 points – To speech
- 2 points – To pain
- 1 point – None
- Verbal Response
- 5 points – Oriented
- 4 points – Confused conversation
- Not sure where they are, or what their name is
- 3 points – Inappropriate words
- They speak real words, but they are not in context
- 2 points – Incomprehensible sounds
- 1 point – None
- Motor Response
- 6 points – Obeys commands
- 5 points – Localizes to pain
- Crosses midline/clavicles to remove painful stimuli
- 4 points – Withdrawal to pain
- Moves extremity/head away from painful stimuli
- 3 points – Decorticate (flexor) posturing
- 2 points – Decerebrate (extensor) posturing
- 1 point – None
Our patient’s score is 3E + 4V + 5M = 12
How good is it?
The GCS was never designed to be used for acute injury. It was created to monitor changes in neurologic status of patients in a neurosurgical unit and was not designed to have the 3 individual variables combined into one score. Here are the important limitations of the GCS.
- The GCS is NOT reliable
- It is made up of subjective elements that are open to the interpretation of each provider assessing the patient and has been repeated shown to have poor inter-rater reliability.
- One study showed only a 38% accuracy between raters and were 2 or more points off 33% of the time.
- Providers CAN’T remember the scale
- It has too many elements and is regarded as too complicated to be easily, and rapidly applied to patients
- In 2003, it was discovered that 25% of British hospitals were using the original 12-point scale instead of the current 13-point scale without anyone noticing.
- The GCS is only GROSSLY predictive
- It is not designed to predict outcomes of patients with acute neurologic injury.
- The GCS is NOT equal to the sum of its parts
- The original creators vehemently opposed the summed total score because it assumes that each variable is equal to the others in terms of importance
- Example
- GCS of 4 with 1E + 1V + 2M = 48% mortality
- GCS of 4 with 1E + 2V + 1M = 27% mortality
- GCS of 4 with 2E + 1V + 1M = 19% mortality
Are there any other scoring systems out there?
The motor subscale of the GCS has been proven to be most predictive of outcomes in patients with neurologic trauma and injury. This has led to debate about whether to do away with the other 2 subscales and use just the motor score (since it has been shown to close to linear in regards to survival).

Healy C. J Trauma. 2003.
But this is still 6 points and some argue can be further simplified. One study broke down the 6-point motor subscale and found that only 3 of those were statistically important. Those are:
- Obeys commands
- Localizes to pain
- Withdrawal to pain or less
This new Simplified Motor Scale can be remembered by the acronym TROLL (Test Responsiveness: Obeys, Localizes, Less). 2 other simplified scores have also been created to help quickly determine neurologic status. These are:
- AVPU
- Alert
- Responds to verbal stimuli
- Responds to painful stimuli
- Unresponsive
- ACDU
- Alert
- Confused
- Drowsy
- Unresponsive
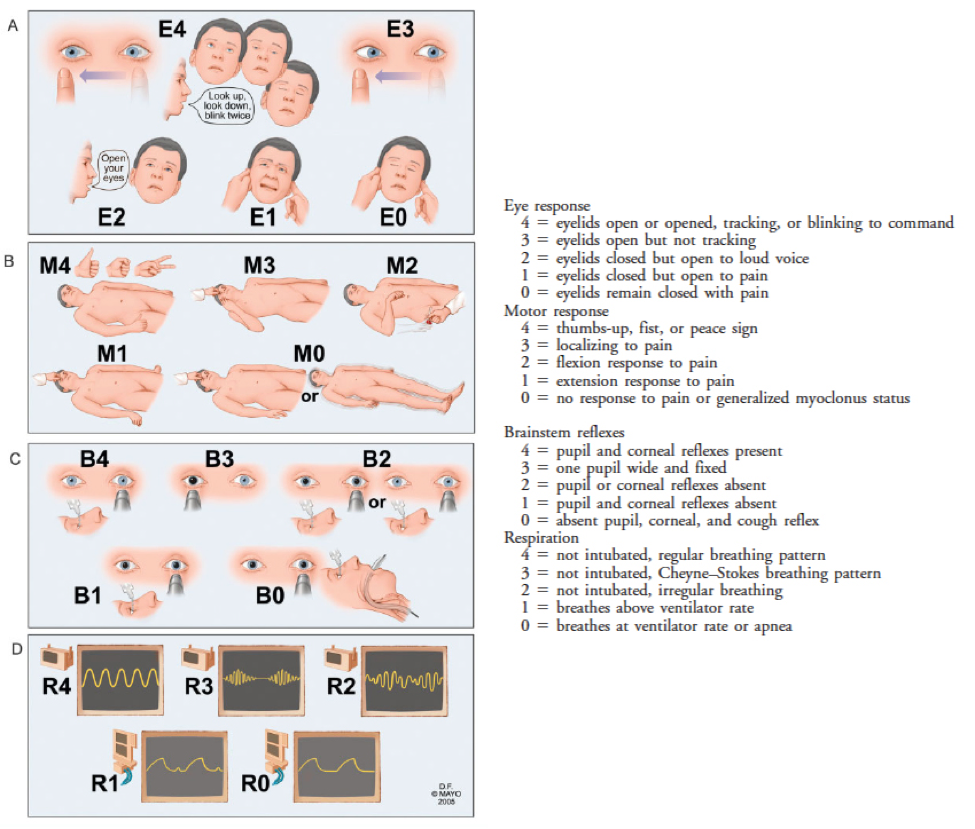
There is another, although more complicated, score called the FOUR score, which has 4 components and stands for Full Outline of UnResponsiveness. Unfortunately, it is even more complicated than the GCS (in the original study it was performed by neurologic specialists, not general practitioners) and it performed just as poorly in external validation studies as the GCS.

Wijdicks EF. Ann Neurol. 2005.
Bottom Line
GCS is essentially worthless clinically even when it is calculated correctly. Simplified scores give just as much information, are easier to use, and are just as predictive. But….you will always be asked “what is the patient’s GCS”, in spite of the growing evidence against it.
References
- Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81-4.
- Green SM. Cheerio, laddie! Bidding farewell to the Glasgow Coma Scale. Ann Emerg Med. 2011;58(5):427-30.
- Teasdale G, Jennett B, Murray L, Murray G. Glasgow coma scale: to sum or not to sum. Lancet. 1983;2(8351):678.
- Zuercher M, Ummenhofer W, Baltussen A, Walder B. The use of Glasgow Coma Scale in injury assessment: a critical review. Brain Inj. 2009;23(5):371-84.
- Healey C, Osler TM, Rogers FB, et al. Improving the Glasgow Coma Scale score: motor score alone is a better predictor. J Trauma. 2003;54(4):671-8.
- Gill M, Windemuth R, Steele R, Green SM. A comparison of the Glasgow Coma Scale score to simplified alternative scores for the prediction of traumatic brain injury outcomes. Ann Emerg Med. 2005;45(1):37-42.
- Mcnarry AF, Goldhill DR. Simple bedside assessment of level of consciousness: comparison of two simple assessment scales with the Glasgow Coma scale. Anaesthesia. 2004;59(1):34-7.
- Wijdicks EF, Bamlet WR, Maramattom BV, Manno EM, Mcclelland RL. Validation of a new coma scale: The FOUR score. Ann Neurol. 2005;58(4):585-93.
- Fischer M, Rüegg S, Czaplinski A, et al. Inter-rater reliability of the Full Outline of UnResponsiveness score and the Glasgow Coma Scale in critically ill patients: a prospective observational study. Crit Care. 2010;14(2):R64.