
82-year-old male, with a history of HTN, HLD, and CAD, presents to your clinic with a six-month history of dyspnea on exertion. He states he is unable to walk as far as he used when exercising, and when he over exerts himself, he reports having some mild chest pain and feeling lightheaded. This resolves with rest and he denies any syncope with these events.
Medications
Metoprolol 50mg daily
Lisinopril 10mg daily
Simvastatin 30mg daily
Vital Signs
BP – 158/97
HR – 62
RR – 13
O2% – 100%
Physical exam
General – WN/WD male in NAD
Pulmonary – CTA without adventitial breath sounds
CV – Soft S2 with murmur over right 2nd intercostal space
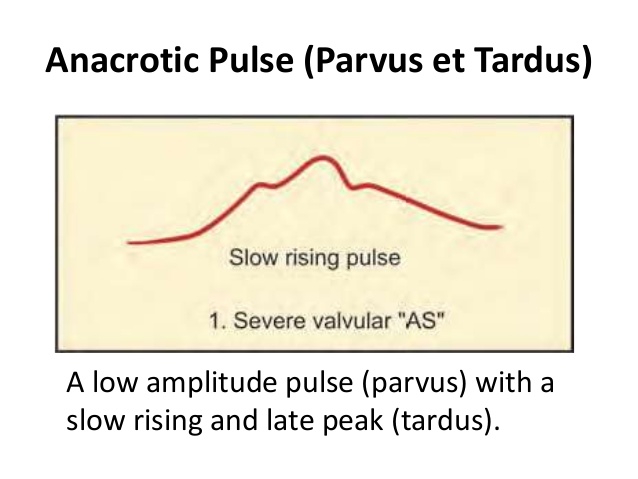
PV – carotid pulse is weak and has a slow rise, murmur is appreciated
Neuro – No focal deficits
EKG

This patient has aortic stenosis. The suggestive parts of the H&P are:
- History
- The classic triad of aortic stenosis is chest pain, dyspnea, and syncope.
- Aortic stenosis increases in prevalence with age
- Cardiac Auscultation
- Soft, single S2 since A2, which is due to aortic valve closure, is delayed and occurs with P2
- Murmur
- Systolic ejection murmur best heard over the right 2nd intercostal space

- Begins on S1 and ends before S2
- May radiate to the carotids

-
- Peripheral Vascular
- Carotid Palpation
- Pulsus Parvus et Tardus (weak and late)

- EKG
- Shows LVH and strain pattern in precordial leads


- What is the next step in the management of this patient?
- Transthoracic echocardiography
- After the next step, what important variables must you specifically assess?
- Valvular anatomy and size
- Aortic valve surface area
- Valve hemodynamics
- Transvavular aortic velocity
- Mean transvalvular pressure
- LV size and ejection fraction
- Pulmonary artery pressure
- Other concomitant conditions
- Valvular anatomy and size
These variables will help with staging the severity of the stenosis, as well as determine need for operative intervention.
