

***LISTEN TO THE PODCAST HERE***
These questions stemmed from an email I got from a former student about electrolyte questions they are getting in the clinical year. These are a quick and basic overview of common electrolyte questions and issues students may see on clinical rotations
#1 – Clinical Repletion of Electrolytes and Monitoring
Not every electrolyte on the chemistry panel needs to be repleted when low…but you need to know which ones can cause problems. The problem children are:
- Potassium
- Calcium
- Magnesium
- Phosphorus
Why? These four can all cause cardiac dysrhythmias when low and why all these should be on telemetry, or at least some basic monitoring, when repleting.
Your first step should ALWAYS ALWAYS ALWAYS be to make sure you know why it is low. Yes, we can keep repleting electrolytes to normal levels, but you will be doing this in perpetuity unless you fix the problem causing it in the first place. Let’s review the major points for each:
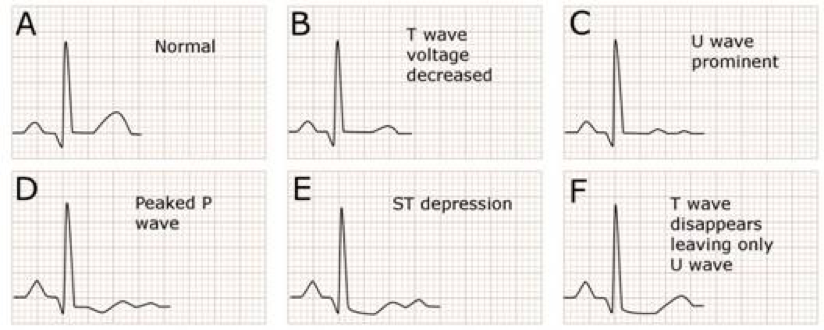
- Hypokalemia
- Major Cause – Diuretics, GI losses
- EKG Changes – Flat T-waves, U-wave. ST-depression

- Repletion Pearls
- Asymptomatic
- Oral replacement – KCl 10-40 mEq 2-4 times per day
- Symptomatic
- IV replacement – KCl 20-40 mEq/L at 10 mEq/hr
- Asymptomatic
- Hypocalcemia
- Major Cause – Diuretics, Hypoparathyroidism, CKD
- EKG Changes – Prolonged QT

- Repletion Pearls
- Asymptomatic
- Oral elemental calcium 1500-2000 mg/day
- Symptomatic
- IV calcium gluconate 1-2g in 50mL D5W
- IV calcium chloride 1000mg in 10mL D5W
- Asymptomatic
- Hypomagnesemia
- Major Causes – GI losses, Diuretics
- EKG Changes – QRS widening, peak T-wave, prolongation PR
- Repletion Pearls
- Asymptomatic
- Oral magnesium salts 240-1000mg 2-4 times/day
- Symptomatic
- IV MgSO4 1-8g
- Asymptomatic
- Hypophosphatemia
- Major Causes – Hyperparathyroidism, Refeeding Syndrome, Hungry Bone Syndrome
- Major Sequelae – ATP depletion, hemolysis

- Repletion Pearls
- Asymptomatic
- Oral sodium/potassium phosphate 30-80 mmol/day
- Symptomatic
- IV sodium/potassium phosphate 10-40 mmol/day
- Asymptomatic



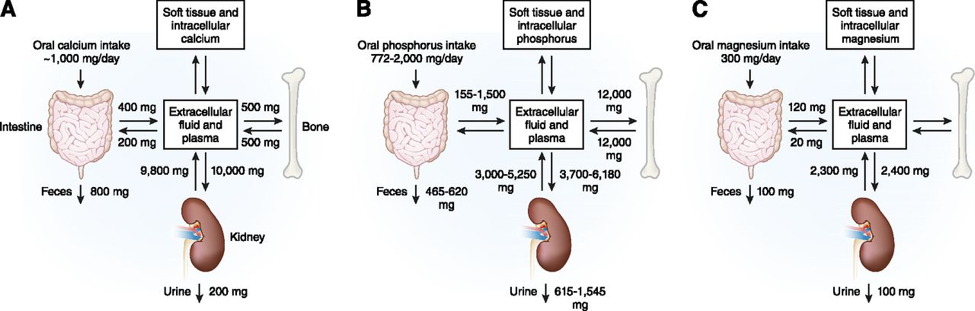
#2 – Calcium/Magnesium/Phosphorus Relationship
You must have a good understanding of this relationship when managing electrolyte deficiencies because you may not be able to make any headway on one if you don’t fix the other.

- Magnesium and Calcium/Potassium
- Hypomagnesemia causes functional hypoparathyroidism by inducing PTH resistance and decreasing calcium secretion and increasing calcium excretion.
- Hypomagnesemia also causes cellular expression of ROMK channels in the nephron which increase potassium excretion
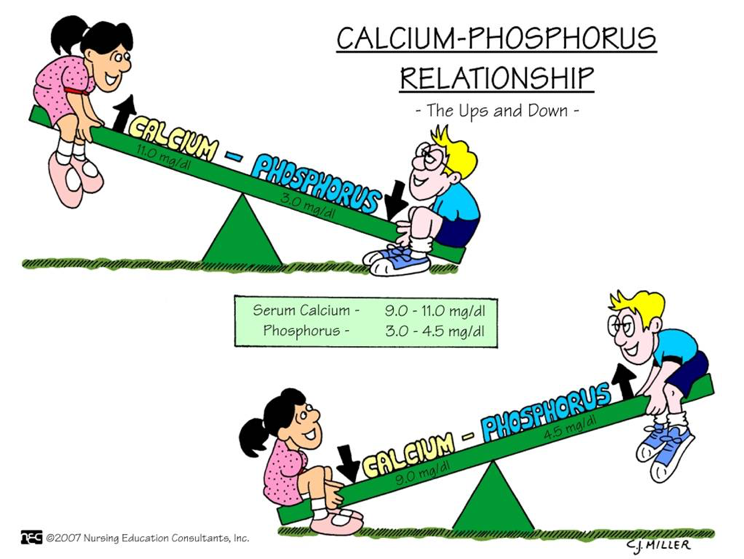
- Calcium and Phosphorus
- There is an inverse relationship between calcium and phosphorus because of PTH. As PTH increases (seen as a response to hypocalcemia), there is an increase in phosphorus excretion
#4 – Hyponatremia Pearls
Hyponatremia is actually really easy to work up. If you find you patient has a low sodium, check a serum osmolarity, urine osmolarity, and urine sodium.

References
- Maday KR. Understanding electrolytes: important diagnostic clues to patient status. JAAPA. 2013; 26(1):26-31. [pubmed]
- Gennari FJ. Hypokalemia. NEJM. 1998; 339(7):451-8. [pubmed]
- Cooper MS, Gittoes NJ. Diagnosis and management of hypocalcaemia. BMJ. 2008; 336(7656):1298-302. [pubmed]
- Agus ZS. Hypomagnesemia. JASN. 1999; 10(7):1616-22. [pubmed]
- Gaasbeek A, Meinders AE. Hypophosphatemia: an update on its etiology and treatment. AJM. 2005; 118(10):1094-101. [pubmed]
- Huang CL, Kuo E. Mechanism of hypokalemia in magnesium deficiency. JASN. 2007; 18(10):2649-52. [pubmed]
- Blaine J, Chonchol M, Levi M. Renal control of calcium, phosphate, and magnesium homeostasis. CJASN. 2015; 10(7):1257-72. [pubmed]
- Adrogué HJ, Madias NE. Hyponatremia. NEJM. 2000; 342(21):1581-9. [pubmed]

Pingback: Electrolyte Essentials | Wilco Wellness