*** LISTEN TO THE PODCAST HERE ***




***LISTEN TO THE PODCAST HERE***

***LISTEN TO THE PODCAST HERE***

Bonney Test
Other Known Aliases – none
Definition – bedside test with urinary incontinence to determine if it is due to anatomical or structural issues
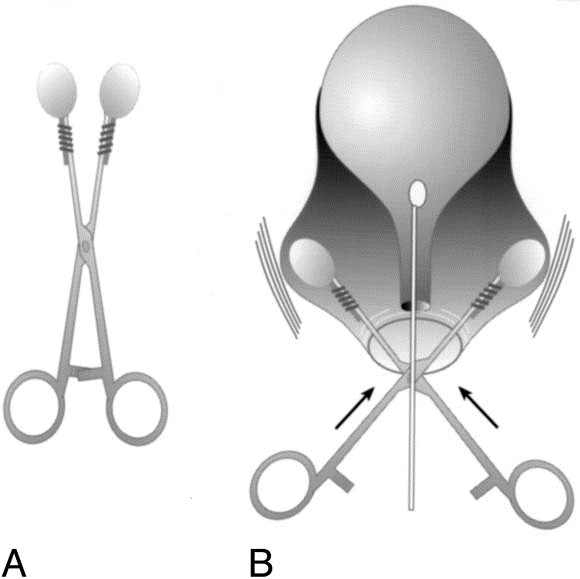
Clinical Significance – After a positive stress incontinence test, Bonney test is performed, where either a specialized instrument or examiner’s fingers are placed laterally to the urethral opening and pushed up to elevate the neck of the bladder. The patient then coughs to see if urine still escapes. If no urine leaks, then the incontinence is due the descent of the bladder neck into the vagina. If urine still escapes, it is due to weakness in the sphincter.
History – Named after William Francis Victor Bonney (1872-1953), a British gynecologist who received his medical doctorate from Chelsea Hospital for Women in 1896. He would go on to achieve Master of Surgery distinction in 1899 and was accepted as a fellow in the Royal College of Surgeons and Physicians in 1900. He would spend his entire career developing, pioneering, and mastering operative techniques in gynecologic surgery towards more conservative approaches to reduce mortality, morbidity, and disability associated with the more conventional approaches of the time. This was largely due to his wife, Annie, receiving a total hysterectomy early in their marriage for anemia associated with her heavy cycles. He also developed his own antiseptic solution called “Bonney’s Blue” used during vaginal surgeries which profoundly reduced infectious mortality. He would author more than 200 manuscripts during his career culminating his Textbook of Gynaecologic Surgery that is still in print today. He is regarded as one of, if not the, major influencer in modern gynecologic surgery.

References

***LISTEN TO THE PODCAST HERE***














Question
This one is a quick one this week. When evaluating a patient with testicular pain (either acute or chronic), what are the specific physical examination techniques you can perform and what conditions do they help rule in/out?
Answer

Sertoli Cells
Other Known Aliases – none
Definition – sustentacular cell of the convoluted seminiferous tubule of the testes
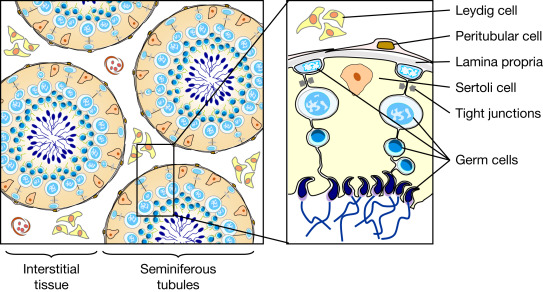
Clinical Significance – these cells are activated by FSH to produce and mature sperm during spermatogenesis
History – Named after Enrico Sertoli (1842-1910), who was an Italian physiologist and histologist and received his medical doctorate from the University of Pavia in 1865. His love and passion for histology was groomed while training under Eusebio Oehl, who was an early pioneer in microscopic anatomy and histopathology. He would go on to become professor of anatomy and physiology at the Royal School of veterinary medicine in Milan and it was here that he founded the laboratory of experimental physiology. In 1865, during his tenure in Milan, he published the paper describing his eponymous cell.

References

Question
This one is a quick one this week. When evaluating a patient with testicular pain (either acute or chronic), what are the specific physical examination techniques you can perform and what conditions do they help rule in/out?
Fournier’s Gangrene
Other Known Aliases – none
Definition – necrotizing fasciitis of the external genitalia and/or perineum
Clinical Significance – this infection commonly affects older men and is associated with diabetes mellitus or a compromised immune system. Other risk factors include trauma or surgery to the perineal area, alcoholism, and childbirth. Pain, erythema, crepitus, and fever are common findings and treatment is aggressive surgical debridement and antibiotics to cover anaerobic and facultative pathogens.
History – Named after Jean Alfred Fournier (1832-1914), who was a French dermatologist and venereologist, and received his medical doctorate in 1860 while studying in Paris. He would begin his career as an understudy of Philippe Ricord at the Hôpital du Midi and would later become médecine des hôpitaux at the famed Hôtel-Dieu de Paris. It was in 1883 when he presented a case series of patients with gangrene of perineum and for which this eponym is attributed, although it was first described and published in 1764 by Baurienne. He is best known for his work with congenital syphilis (for which he has two additional eponyms) and advancing the study of venereal diseases and their connection to degenerative diseases.
References

