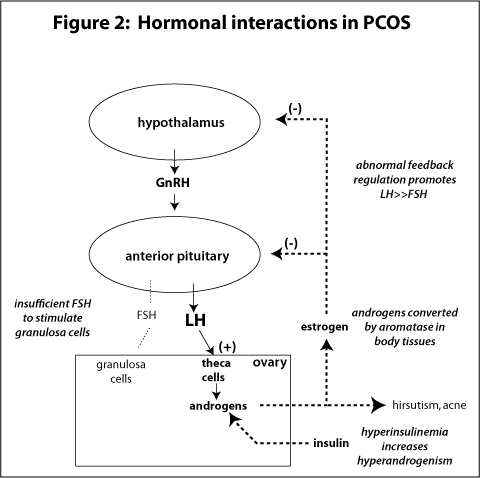
Polycystic ovarian syndrome (PCOS) can often be a clinical diagnosis due to the classic distinguishing features of hirsutism, obesity, menstrual irregularities, and infertility. What is the classic relationship between FSH and LH in a patient with PCOS?
Answer
The classic relationship between LH and FSH in PCOS is > 2.5:1.
LH secretion is elevated, while FSH secretion is the same, or even decreased. LH stimulates theca cell proliferation and secretion of androgens, but there is insufficient FSH to stimulate granulosa cells. Although this is classically seen, LH:FSH is NOT used in any diagnostic criteria for PCOS.
Clinical Significance – Most commonly arising from a gastric adenocarcinoma, but can occur from any metastatic cancer. 80% are bilateral and commonly manifest as pelvic pain, bloating, ascites, or dysparunea. Occasionaly, these tumor can be hormone producing and cause abnormal menstrual bleeding, hirsuitism, or virilization.
History – Named after Friedrich Ernst Krukenberg (1871-1946), who was a German physician and received his medical doctorate from the University of Marburg. He was actually studying to become a ophthalmologist, when he happend to be spending time in the pathology lab under Felix Marchand. It was in this department that Krukenberg described a fibrosarcoma of the ovary (using sections from tumors Marchand had found in 1879) and published his findings in an article entitled “Über das Fibrosarcoma ovarii mucocellulare (carcinomatodes)” in 1896 at the age of 25 as part of his doctoral thesis. He spent the rest of career in his hometown of Halle, Germany practicing as a ophthalmologist.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
American College of Obstetrics and
Gynecology (ACOG) recommends:
All women should be offered
screening before 20 weeks
All women should have the option for
having a more invasive procedure instead of screening regardless of maternal
age
Amniocentesis
Chorionic villus sampling
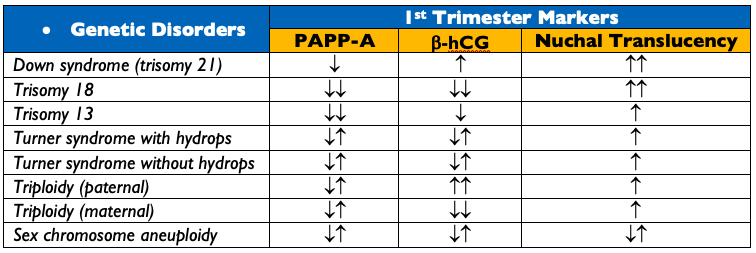
Two major categories of screening
available
Specific maternal serum biomarkers
Primarily trisomy 21 and 18
Maternal circulation cell-free DNA
More sensitive
Assesses trisomy 21, 18, 13, and sex
chromosome aneuploidies
Carrier Screening
ACOG recommends:
All women should be offered carrier
screening for cystic fibrosis, spinal muscular dystrophy, thalassemias, and
hemoglobinopathies
Fragile X
All women with a family history of
intellectual disability, developmental delay, or autism
Each provider develop a screening
strategies for ethnic-specific and panethnic populations
If there is a (+) screening test in
the mother, then the reproductive partner should be offered screening
Standard Panel Laboratory Screening
ABO and Rh Screen
RhD(-) women should receive prophylactic anti(D)-immune globin at 28-weeks
Complete Blood Count and RBC Indices
1st Screen for anemia
Documentation of Rubella and Varicella Immunity
Rubella IgG
Varicella IgG
Urinalysis and Urine Culture
Urine Protein – establish baseline to compare if patient develops pre-eclampsia or eclampsia
Untreated, asymptomatic has higher rates of developing pyelonephritis, pre-term birth
HIV Screen
ACOG recommends “opt-out” approach
Hepatitis B
HBsAg regardless of immunization status
Chlamydia
Nucelic Acid Amplification Test (NAAT) of endocervical/vaginal swab or urine
Syphilis
Can screen with either a non-treponemal or treponemal test, but a (+) screening test is confirmed with a treponemal test
Selective Screening in 1st
Trimester
Thyroid Function – TSH only
Overt diabetes screening
Obtain HgbA1C if BMI > 25 (23 in Asian Americans) AND at least one of the
following:
Gestational diabetes in previous pregnancy
HgbA1C > 5.7%, impaired glucose
tolerance, or impaired fasting glucose on previous testing
1st degree relative with
diabetes
African-American, Latino, Native
American, Asian American, Pacific Islander
History of cardiovascular disease
Hypertension (> 140/90 or on
medication)
Age > 40yr
HDL cholesterol < 35 mg/dL or
triglyceride > 250 mg/dL
PCOS
Physical inactivity
Other insulin resistance conditions
If HgbA1C > 6.5%, then treat as
overt diabetes
If HgbA1C (-), then screen again at
24-28 weeks
Infections
Gonorrhea
NAAT from endocervical/vaginal swab
Hepatitis C
High risk patient should be screened
with anti-HCV antibody or HCV RNA
Tuberculosis
Screen with tuberculin skin test or
interferon-gamma release assay (IGRA) only if:
Suspicion for recent TB infection
Immunocompromised
Others
Toxoplasmosis, trichomonas, herpes
simplex, cytomegalovirus, Zika, and Chagas are available for at risk patients
or in endemic regions
Lead
Women with symptoms of lead exposure
or risk factors
15-24 Weeks
These are not universal and are
options available to mothers
Quadruple Test
Maternal serum alpha-fetoprotein
level
Unconjugated estriol
Human chorionic gonadotropin
Inhibin A
Fetal ultrasound
Can be used to screen for neural
tube defects and other fetal anomalies, as well as screen the mother for a
short cervical length (< 25mm) that can increased her risk of spontaneous
preterm birth
24-28 Weeks
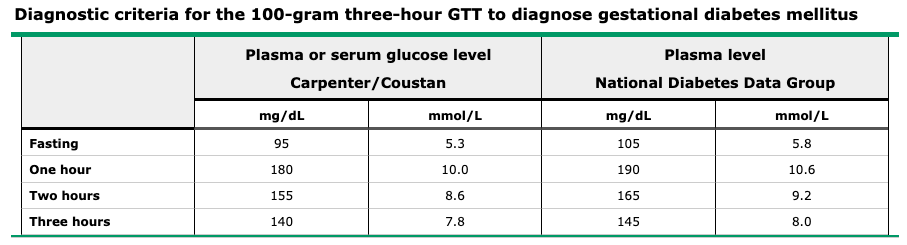
Gestational Diabetes Screening
Two-Step Approach
Step One – Screening
50g, one-hour glucose challenge test REGARDLESS of time of day or last meal
Step Two – Diagnostic
100g, three-hour oral glucose tolerance test
Traditionally diagnostic after 2 elevated values, but newer data suggests that one may be OK
75g, two-hour oral glucose tolerance test
Diagnostic after a single elevated value, but patient must be fasting
Up-To-DateUp-To-Date
Complete Blood Count with iron and
folate studies
2nd anemia screening
28-36 Weeks
Sexually Transmitted Infection
Screening
HIV, syphilis, chlamydia, gonorrhea,
hepatitis B and C
Based on either previous (+) result
or evidence of risk factors
Up-To-Date
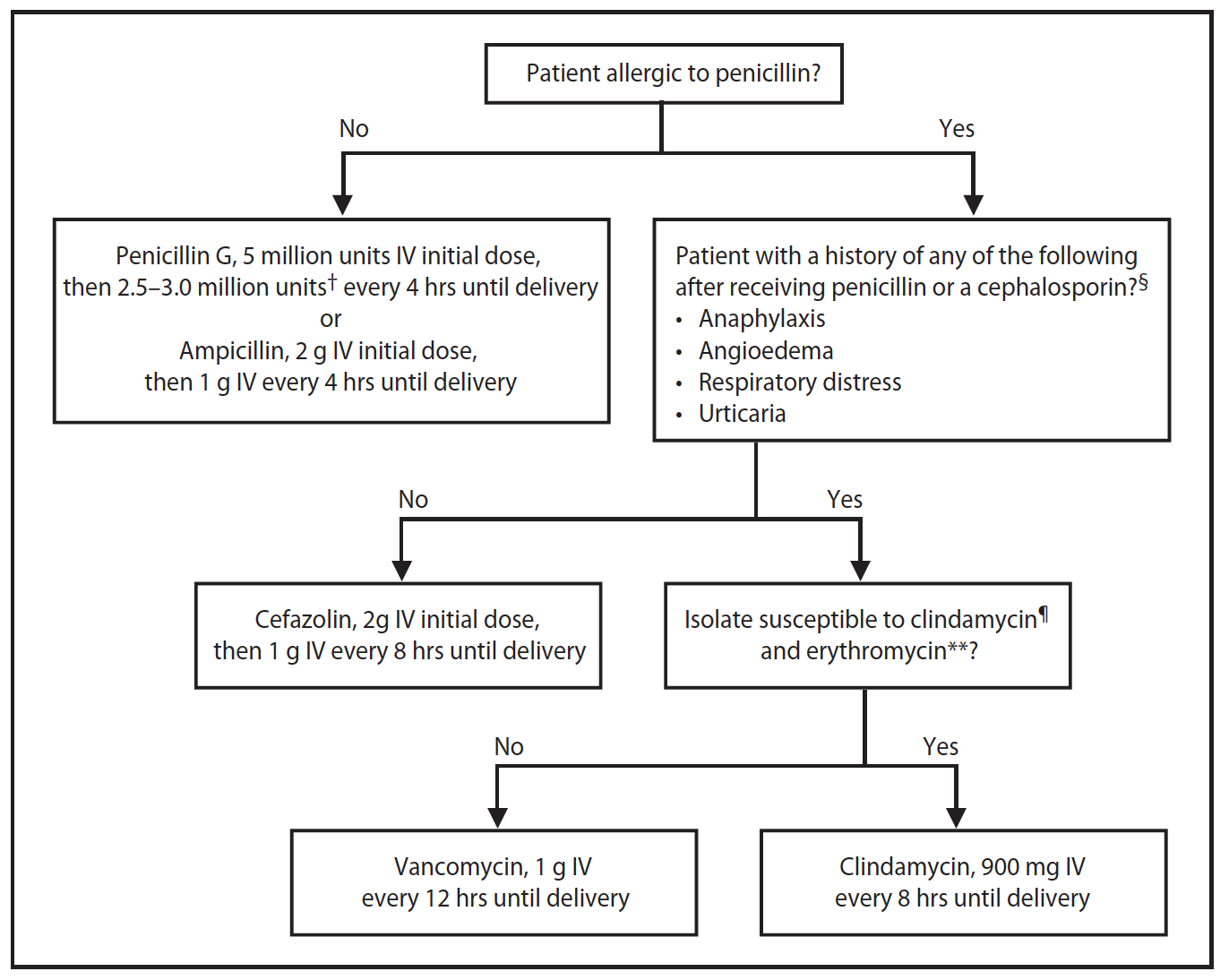
Screen for group B beta-hemolytic
streptococcus
Vaginal and rectal swabs
(+) results treated with intrapartum
prophylaxis
CDC – GBS Prophylactic Antibiotic Algorithm
Screen for Fetal Growth Restrictions
(<10th percentile weight for gestational age)
Indicated in third trimester in
pregnancies at high risk
ACOG Practice Bulletin No. 77: screening for fetal chromosomal abnormalities. Obstetrics and gynecology. 2007; 109(1):217-27. [pubmed]
ACOG Practice Bulletin No. 88, December 2007. Invasive prenatal testing for aneuploidy. Obstetrics and gynecology. 2007; 110(6):1459-67. [pubmed]
ACOG Committee Opinion No. 752: Prenatal and Perinatal Human Immunodeficiency Virus Testing. Obstetrics and gynecology. 2018; 132(3):e138-e142. [pubmed]
Roberts SW, Sheffield JS, McIntire DD, Alexander JM. Urine screening for Chlamydia trachomatis during pregnancy. Obstetrics and gynecology. 2011; 117(4):883-5. [pubmed]
Hughes BL, Page CM, Kuller JA. Hepatitis C in pregnancy: screening, treatment, and management. American journal of obstetrics and gynecology. 2017; 217(5):B2-B12. [pubmed]
ACOG Practice Bulletin No. 190: Gestational Diabetes Mellitus. Obstetrics and gynecology. 2018; 131(2):e49-e64. [pubmed]
Bricker L, Medley N, Pratt JJ. Routine ultrasound in late pregnancy (after 24 weeks’ gestation). The Cochrane database of systematic reviews. 2015; [pubmed]
Polycystic ovarian syndrome (PCOS) can often be a clinical diagnosis due to the classic distinguishing features of hirsutism, obesity, menstrual irregularities, and infertility. What is the classic relationship between FSH and LH in a patient with PCOS?
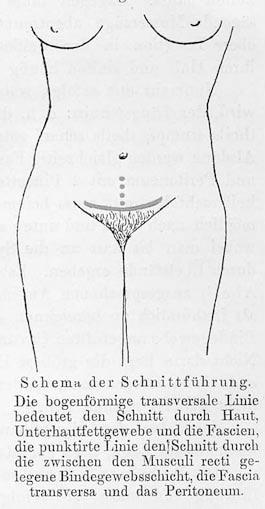
Definition – 8-10cm transverse (slightly arched) incision made 2-3cm cephalad to the pubic symphasis. The rectus sheath is then retracted cephalad and the rectus abdominis muscle bellies are divided longitudinally to enter the peritoneum
Clinical Significance – This is the primary incision for cesarean sections because it follows the Langer Lines and can achieve excellent cosmetic results. There are also decreased rates of postoperative pain, fascial dehiscence, and incisional hernias noted.
History – Named after Hans Hermann Johannes Pfannensteil (1862-1909), who was a German gynecologist and received his medical doctorate from the University of Berlin in 1885. He was an extraordinary surgeon and teacher and published extensively on many gynecological conditions. In 1900, he published an article describing the the advantages of his eponymous transverse fascial incision for gynecologic laparotomies. Dr. Pfannensteil unfortunately died from septicemia at the age of 47 after injuring his finger draining a tubo-ovarian abscess.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Pfannenstiel HJ. (On the advantages of the symphyseal transverse fascial incision for gynecological caliotomies as well as the contribution to the surgical indications). Samml Klin Vortr. 1900;268:1735-56
You have just assisted with a relatively uneventful spontaneous vaginal delivery of a 38-week newborn to a 29-year-old G1P0001 mother. During your immediate, postpartum maternal assessment, you notice a large amount of vaginal bleeding persisting.
Questions
What is the most common cause of this condition?
What are the two most important steps in managing this?
What are some of the other etiologies to think about?
Answers
The most common cause of post-partum hemorrhage is uterine atony and is responsible for up to 75% cases. The amount of bleeding can also be much greater than what is visible due to the flaccid and dilated uterus.
The two most important steps in managing uterine atony are:
Performing bi-manual uterine massage to stimulate contraction
Administration of uterotonics
ALL women get oxytocin either:
15 units in 250mL of LR
10 units IM
If still bleeding after oxytocin:
Carboprost tromethamine (Hemabate) 0.25mg IM every 15min up to a max dose of 8mg
Methergine 0.2mg IM every 2-4 hours
Misprostol 400mcg (SL/buccal/rectal)
Uterine atony is the most common cause of post-partum hemorrhage, but is responsive to uterotonics in most instances, so it is not the most common cause of massive transfusion. Other etiologies to think about are:
Retained placenta/membranes
Lacerations or rupture
HELLP syndrome
Abnormal placentation
References
Bateman BT, Berman MF, Riley LE, Leffert LR. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesthesia and analgesia. 2010; 110(5):1368-73. [pubmed]
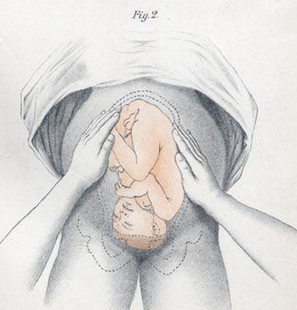
Definition – Series of four distinct actions to systematically determine the lie and position of the fetus in utero:
First Maneuver – Fundal Grip
used to locate fetal position (breech vs vertex)
Second Maneuver – Umbilical Grip
used to locate the back of the fetus
Third Maneuver – Second Pelvic Grip
used to determine pelvic inlet position
Fourth Maneuver – First Pelvic Grip
used to locate the fetal brow
Clinical Significance – These are now an antiquated way to determine fetal positioning to predict difficult deliveries or need for cesarean section. These have largely been replaced by obstetrical ultrasound.
History – Named after Christian Gerhard Leopold (1846-1911), who was a German gynecologist and received his medical doctorate from the University of Leipzig in 1870. He spent the early part of his career teaching midwifery at the Frauenklinik in Leipiz before taking a professorship at the University of Leipzig in 1883. Later that same year, he took over as the Director of the Dresden Royal Gynaecological Infirmary and by the end of his tenure developed it into a leading hospital in Germany. He published his eponymous maneuvers in several articles (first in 1894) in the journal Archiv für Gynäkologie, for which he was a co-editor.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
You have just assisted with a relatively uneventful spontaneous vaginal delivery of a 38-week newborn to a 29-year-old G1P0001 mother. During your immediate, postpartum maternal assessment, you notice a large amount of vaginal bleeding persisting.
Questions
What is the most common cause of this condition?
What are the two most important steps in managing this?
What are some of the other etiologies to think about?
Definition – systolic precordial crunching sound that occurs with each contraction of the heart that is best heard over precordium in the left lateral decubitus position
Clinical Significance – this is one of the classic physical examination findings in pneumomediastinum or pneumopericardium as a result of trauma to the bronchial tree, bleb rupture, or esophageal rupture.
History – Named after Louis Virgil Hamman (1877-1946), an American internists who received his medical doctorate from Johns Hopkins University in 1902. He was considered one of the great physicians of his era and made significant progress in the management of tuberculosis as the head of the Phipps Tuberculosis Clinic at Johns Hopkins. He described this finding in patients with spontaneous mediastinal emphysema in two separate articles, first in 1939 in The Bulletin of Hopkins Hospital, and then in JAMA in 1945.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.