

*** LISTEN TO THE PODCAST HERE ***
Pathophysiology
- Motor gut disorder characterized by failure of the neural crest cells (which are precursors to the enteric ganglion cells) to fully migrate to the distal portions of the colon.
- Most accepted theory is there is a defect in the craniocaudal migration of neuroblasts that occurs between 4-7 weeks gestation
- 12 genetic mutations currently identified predominantly affecting the RET proto-oncogene
- Produces a tyrosine kinase protein that transduces growth and differentiation signals in developing tissues
- 12 genetic mutations currently identified predominantly affecting the RET proto-oncogene
- Most accepted theory is there is a defect in the craniocaudal migration of neuroblasts that occurs between 4-7 weeks gestation
- The absence of these cells in the mucosal and muscular layer of the colon results in the failure of the colonic muscles to relax.

Epidemiology
- Occurs in 1:5000 live births
- Male:Female ratio of 3-4:1
- 80% of cases affect the rectosigmoid junction (termed short-segment disease)
- 15-20% of cases extend to the proximal sigmoid colon (termed long-segment disease)
- <5% of cases affect the entire colon
Associated Syndromes
- Trisomy 21(up to 16% of cases)
- Bardet-Biedi
- Cartilage-hair hypoplasia
- Congenital central hypoventilation syndrome
- Familial dysautonomia
- Multiple endocrine neoplasia type 2
- Mowat-Wilson
- Smith-Lemli-Opitz
- Waardenburg
Associated Congenital Anomalies
Up to 25% of Hirschsprung patients have other congenital anomalies including:
- Genitourinary (20-40%)
- Hydronephrosis, renal agenesis
- Visual/Hearing Impairment (5-40%)
- Most are refractive errors
- Congenital Heart Disease (50%)
- Almost exclusively in syndromic Hirschsprung
- Anorectal Malformations
Signs and Symptoms
- Failure to pass meconium in first 48 hours
- 100% of normal full-term infants pass meconium in first 48 hours in contrast to only 10-40% of infants with Hirschsprung
- Abdominal distention
- Squirt/Blast Sign
- Explosive expulsion of gas and stool after digital rectal examination
- Squirt/Blast Sign
- Bilious emesis
- Enterocolitis and volvulus are rare, life-threatening complications or presentations
- Most are diagnosed in the neonatal period, but less-severe short-segment disease can present as late as 3 years old
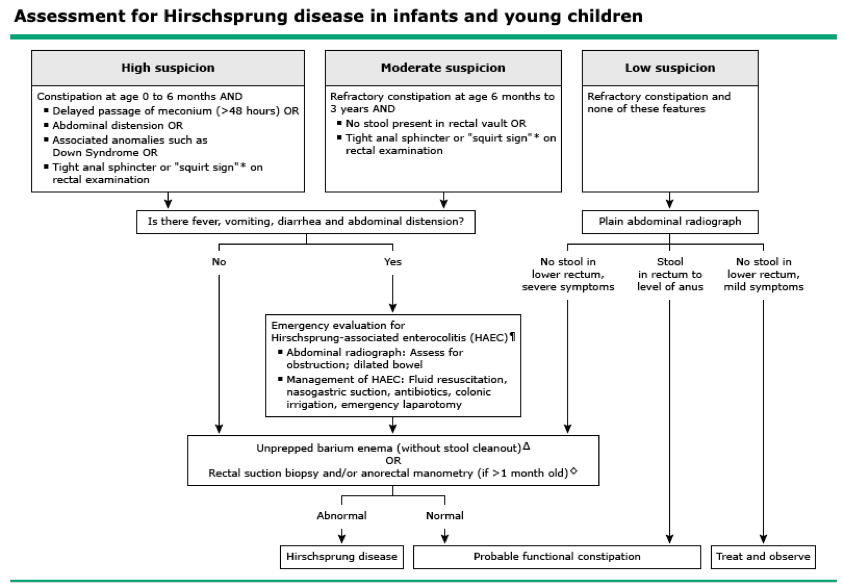
Diagnostic Work-Up
- Indications for testing include:
- Symptoms of obstruction
- Failure to pass meconium after 48 hours
- Constipation and Trisomy 21 (or other associated syndrome)
- Constipation and physical examination suggestive of Hirschsprung
- If fever, lethargy, and/or obstipation are present, emergent evaluate for enterocolitis is needed
- Studies
- “Unprepped” contrast enema
- Identification of transition zone
- Change from normal caliber/narrowed rectum to dilated proximal colon
- Identification of transition zone
- “Unprepped” contrast enema

- Anorectal manometry
- Useful in ultrashort segment disease
- Can approach 100% NPV is performed properly
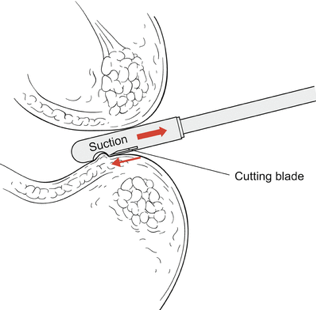
- Suction rectal biopsy
- GOLD STANDARD for diagnosis
- Location should be 2cm above the level of the dentate line
- Histology findings
- Presence of hypertrophic nerve fibers
- Increased acetylcholinesterase activity or staining in the muscularis mucosae
- Decreased or absent calretinin-immunoreactive fibers in the lamina propria

Treatment
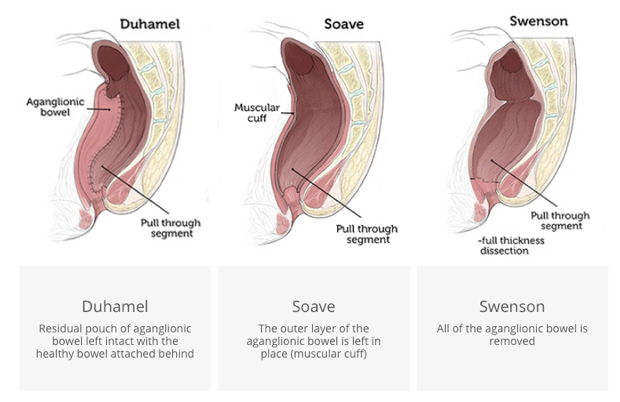
- Surgery is the mainstay of treatment
- Resect the affected segment
- Bring the normal ganglionic bowel down to anus
- Preserve internal sphincter function
- Originally, this was an open, two-stage procedure with a diverting colostomy
- To allow the dilated segement to decompress back to normal size
- Now, it can be performed as a single-stage operation either laparoscopically or transanally
- 3 types of Pull-Through Procedures
- Complications
- Anastomotic stricture, constipation, incontinence, or enterocolitis
The Cottage Physician (1893)

References
- Hoffenberg EJ, Furuta GT, Kobak G, Walker T, Soden J, Kramer RE, Brumbaugh D. Gastrointestinal Tract. In: Hay, Jr. WW, Levin MJ, Deterding RR, Abzug MJ. eds. Current Diagnosis & Treatment: Pediatrics, 24e New York, NY: McGraw-Hill
- Badner JA, Sieber WK, Garver KL, Chakravarti A. A genetic study of Hirschsprung disease. American journal of human genetics. 1990; 46(3):568-80. [pubmed]
- Fu M, Tam PK, Sham MH, Lui VC. Embryonic development of the ganglion plexuses and the concentric layer structure of human gut: a topographical study. Anatomy and embryology. 2004; 208(1):33-41. [pubmed]
- Goldstein AM, Hofstra RM, Burns AJ. Building a brain in the gut: development of the enteric nervous system. Clinical genetics. 2013; 83(4):307-16. [pubmed]
- Amiel J, Sproat-Emison E, Garcia-Barcelo M, et al. Hirschsprung disease, associated syndromes and genetics: a review. Journal of medical genetics. 2008; 45(1):1-14. [pubmed]
- Pini Prato A, Rossi V, Mosconi M, et al. A prospective observational study of associated anomalies in Hirschsprung’s disease. Orphanet journal of rare diseases. 2013; 8:184. [pubmed]
- Sarioglu A, Tanyel FC, Büyükpamukçu N, Hiçsönmez A. Hirschsprung-associated congenital anomalies. European journal of pediatric surgery : official journal of Austrian Association of Pediatric Surgery … [et al] = Zeitschrift fur Kinderchirurgie. 1997; 7(6):331-7. [pubmed]
- Khan AR, Vujanic GM, Huddart S. The constipated child: how likely is Hirschsprung’s disease? Pediatric surgery international. 2003; 19(6):439-42. [pubmed]
- Arshad A, Powell C, Tighe MP. Hirschsprung’s disease. BMJ (Clinical research ed.). 2012; 345:e5521. [pubmed]
- Evaluation and treatment of constipation in infants and children: recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Journal of pediatric gastroenterology and nutrition. 2006; 43(3):e1-13. [pubmed]
- Putnam LR, John SD, Greenfield SA, et al. The utility of the contrast enema in neonates with suspected Hirschsprung disease. Journal of pediatric surgery. 2015; 50(6):963-6. [pubmed]
- Meinds RJ, Trzpis M, Broens PMA. Anorectal Manometry May Reduce the Number of Rectal Suction Biopsy Procedures Needed to Diagnose Hirschsprung Disease. Journal of pediatric gastroenterology and nutrition. 2018; 67(3):322-327. [pubmed]
- Alizai NK, Batcup G, Dixon MF, Stringer MD. Rectal biopsy for Hirschsprung’s disease: what is the optimum method? Pediatric surgery international. 1998; 13(2-3):121-4. [pubmed]
- Hackam DJ, Grikscheit T, Wang K, Upperman JS, Ford HR. Pediatric Surgery. In: Brunicardi F, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE. eds. Schwartz’s Principles of Surgery, 10e New York, NY: McGraw-Hill; 2015
