
***LISTEN TO THE PODCAST HERE***
Epidemiology
- Approximately 5 million people in
the US
- Majority are groin hernias
- 2/3rd are on the right
- Majority are groin hernias
- 1/3rd of all repairs are
ventral hernias
- 1/3rd of these are incisional and 2/3rd are primary
Anatomy
The abdominal wall is made up of multiple, overlapping muscles and connective tissue whose main purpose is to contain and protect the intra-abdominal organs, while also serving as accessary muscles of respiration and facilitating axial movements. The bony boundaries of the abdominal cavity are:
- Xiphoid process superiorly and
costal margins laterally
- With diaphragm separating the abdominal cavity from thoracic cavity
- Pubic symphysis inferiorly and iliac
crests laterally
- With the inguinal ligament connecting them
The lateral rectus abdominis muscles also fuse midline to form the linea alba and laterally to the connect with the confluence of the external oblique, internal oblique, and transverse abdominis muscles.
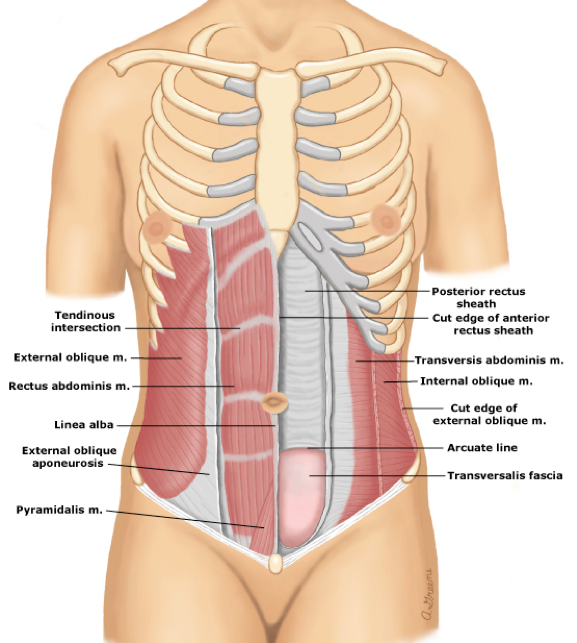
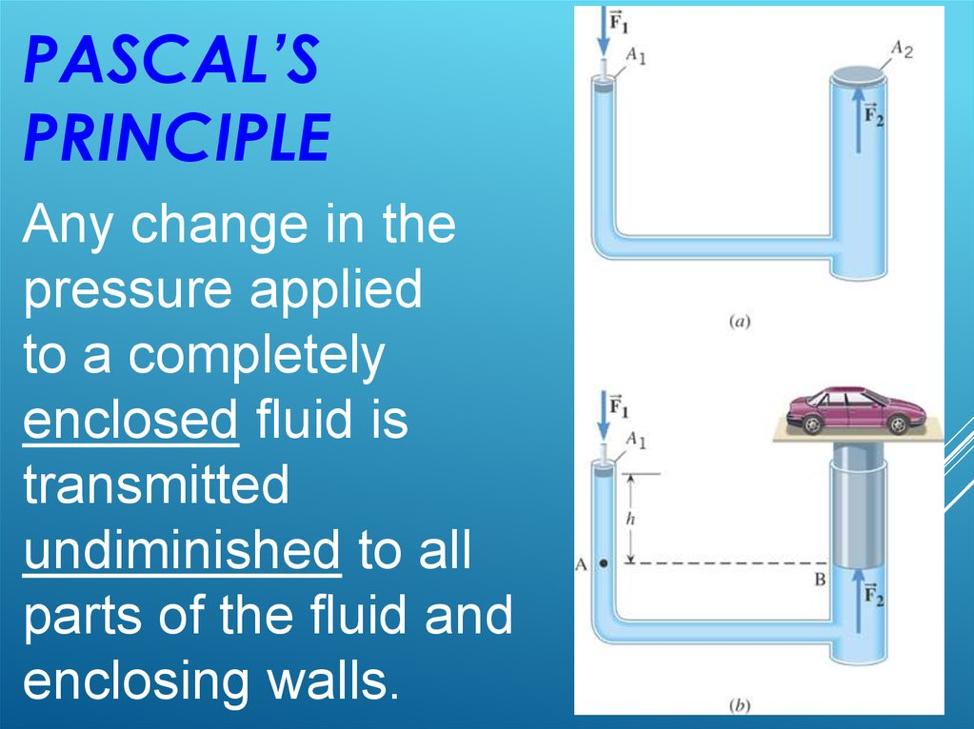
Weakness at any of these junctions (either anatomic or iatrogenic) can allow herniation of abdominal contents through this defect. Pascal’s principle states that any pressure generated within a closed system (abdominal cavity) is transmitted equally to the walls of the system.
Classification and Definitions of Hernia Types
- Ventral
- Anterior
- Epigastric
- Occur between Xiphoid and umbilicus
- Generally < 1cm in size
- Umbilical
- Most common overall and more common in women
- Spigelian
- Occurs through aponeurosis of the transverse abdominal muscle bounded by the linea semilunaris and lateral edge of the rectus muscle medially
- Incisional

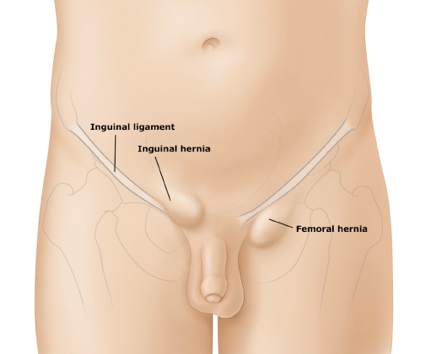
- Groin
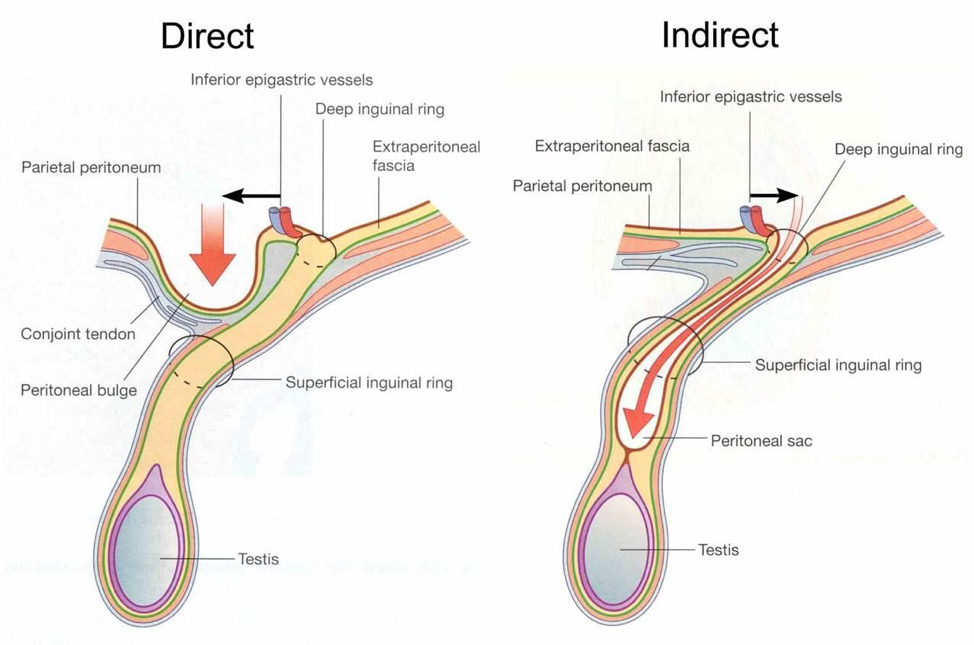
- Inguinal
- Direct
- Weakness of posterior wall of the inguinal canal inferior to the inferior vessels
- Indirect (most common overall)
- Through the deep ring and inguinal canal
- Direct
- Femoral (more common in women)
- Through the femoral ring into the femoral canal posterior and inferior to the inguinal ligament
- Inguinal

Signs and Symptoms
- History
- Can be asymptomatic if small
- Most patients will feel a “bulge” and have varying degree of pain associated with this
- Coughing, straining, or Valsalva worsen the pain or increase the size
- Groin Hernias
- Heaviness or dull discomfort in the groin
- Pain improves when lying supine
- Systemic symptoms (fever, nausea/vomiting, abdominal pain, bloating) should raise your suspicion of an incarcerated or strangulated hernia
- Physical Examination
- Abdominal wall should be examined with the patient standing and lying supine
- Have patient bear down or cough to accentuate while palpating in the anatomic region
- Examine for previous surgical incisions
- Palpate around the umbilicus
- In men, invaginate the scrotal skin to reach the inguinal canal
- Femoral hernias most commonly occur medial to the femoral pulse
- If any erythema or induration is visible, or if the bulge is tender to palpation, this should raise your suspicion of an incarcerated or strangulated hernia
- Abdominal wall should be examined with the patient standing and lying supine

Diagnosis
Most hernias in non-obese patients should be diagnosed by careful and thorough history and physical examination. In others, radiographic investigation must be performed.
- Computed Tomography
- Gold standard to identify sac, contents, and surrounding edema or inflammation


- Ultrasound
- Can be very helpful if the diagnosis of groin hernia is unclear
Surgical Repair
Most hernias will require surgical repair at some point. The decision for operative management comes down to risk of future complications, size, and symptom tolerance. Patients with strangulation or incarceration MUST emergent/urgent surgical repair to limit the risk of bowel ischemia.
Surgeon preference and patient considerations dictate laparoscopic vs open hernia repair.
Preclusion to laparoscopic repair include:
- Prior surgery involving the preperitoneal space
- Complicated hernias
- Ascites
- Inability to tolerate general anesthesia

Surgical Techniques for Groin Hernias
- Open
- Tension-free mesh repairsPrimary tissue approximation non-mesh repair
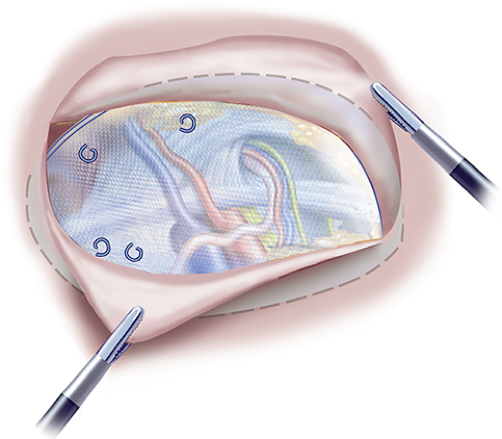
- Laparoscopic (both require mesh)
- Totally extraperitoneal (TEP) repair
- Avoids the peritoneal cavity by developing
a plane of dissection in the preperitoneal space
- Landmarks for entry to the preperitoneal
space are:
- Median umbilical ligament
- Hernia defect
- Landmarks for entry to the preperitoneal
space are:
- This space is entered by establishing a plane between the posterior surface of the rectus muscle and posterior rectus sheath and peritoneum
- Avoids the peritoneal cavity by developing
a plane of dissection in the preperitoneal space
- Totally extraperitoneal (TEP) repair
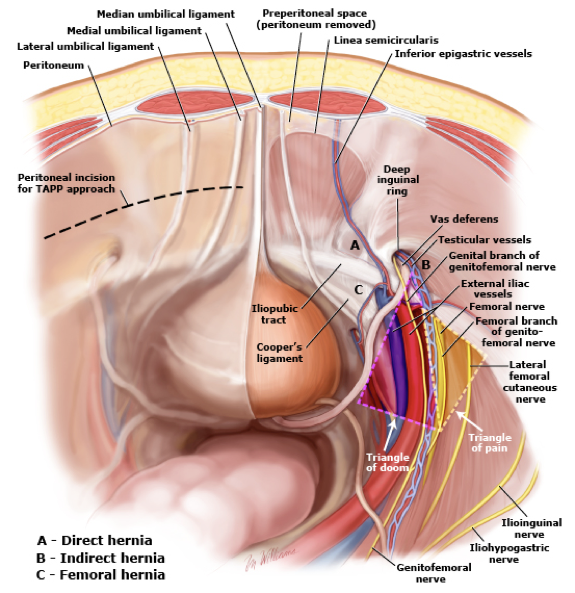
- Transabdominal preperitoneal patch
(TAPP) repair
- Advantage is that all three groin hernia types are well visualized and in close proximity to each other
Surgical Repair for Ventral Hernias
- Goals for repair
- Prevent hernia recurrence
- Low rate of surgical site infection
- Provide dynamic muscle support
- Provide a repair with physiologic tension
- Prevent eventration or abdominal wall bulging
- Incorporate the abdominal wall
- < 1cm
- Open repair with or without mesh directly over the defect
- 1-10cm
- Can be repaired either open or
laparoscopic with mesh
- 1-4cm midline ventral – open
- 1-4cm incisional – open or laparoscopic
- 4-10cm all types – laparoscopic
- Can be repaired either open or
laparoscopic with mesh
- > 10cm
- Unlikely to be closed laparoscopic and require open
Cottage Physician
References
- Park AE, Roth JS, Kavic SM. Abdominal wall hernia. Current problems in surgery. 2006; 43(5):326-75. [pubmed]
- Earle DB, McLellan JA. Repair of umbilical and epigastric hernias. The Surgical clinics of North America. 2013; 93(5):1057-89. [pubmed]
- Flament JB. [Functional anatomy of the abdominal wall]. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen. 2006; 77(5):401-7. [pubmed]
- Ellis H. Applied anatomy of abdominal incisions. British journal of hospital medicine (London, England : 2005). 2007; 68(2):M22-3. [pubmed]
- Rutkow IM. Demographic and socioeconomic aspects of hernia repair in the United States in 2003. The Surgical clinics of North America. 2003; 83(5):1045-51, v-vi. [pubmed]
- McIntosh A, Hutchinson A, Roberts A, Withers H. Evidence-based management of groin hernia in primary care–a systematic review. Family practice. 2000; 17(5):442-7. [pubmed]
- Murphy KP, O’Connor OJ, Maher MM. Adult abdominal hernias. AJR. American journal of roentgenology. 2014; 202(6):W506-11. [pubmed]
- Bedewi MA, El-Sharkawy MS, Al Boukai AA, Al-Nakshabandi N. Prevalence of adult paraumbilical hernia. Assessment by high-resolution sonography: a hospital-based study. Hernia : the journal of hernias and abdominal wall surgery. 2012; 16(1):59-62. [pubmed]
- Earle D, Roth JS, Saber A, et al. SAGES guidelines for laparoscopic ventral hernia repair. Surgical endoscopy. 2016; 30(8):3163-83. [pubmed]
- Sailes FC, Walls J, Guelig D, et al. Synthetic and biological mesh in component separation: a 10-year single institution review. Annals of plastic surgery. 2010; 64(5):696-8. [pubmed]
- Shell DH, de la Torre J, Andrades P, Vasconez LO. Open repair of ventral incisional hernias. The Surgical clinics of North America. 2008; 88(1):61-83, viii. [pubmed]
- Luijendijk RW, Hop WC, van den Tol MP, et al. A comparison of suture repair with mesh repair for incisional hernia. The New England journal of medicine. 2000; 343(6):392-8. [pubmed]
- DiBello JN, Moore JH. Sliding myofascial flap of the rectus abdominus muscles for the closure of recurrent ventral hernias. Plastic and reconstructive surgery. 1996; 98(3):464-9. [pubmed]
