47yo man presents to your clinic to establish care. He has a history of resistant hypertension, DMII, and sleep apnea. Vital signs are BP-159/101, HR-74, RR-16, O2-100%, and temp-98.9. Physical examination is also significant for multiple bruises on the lower extremities.
What would be the next step in the diagnosis of this patient?
What else would you need to order to determine the cause of this patient’s condition?
Answer
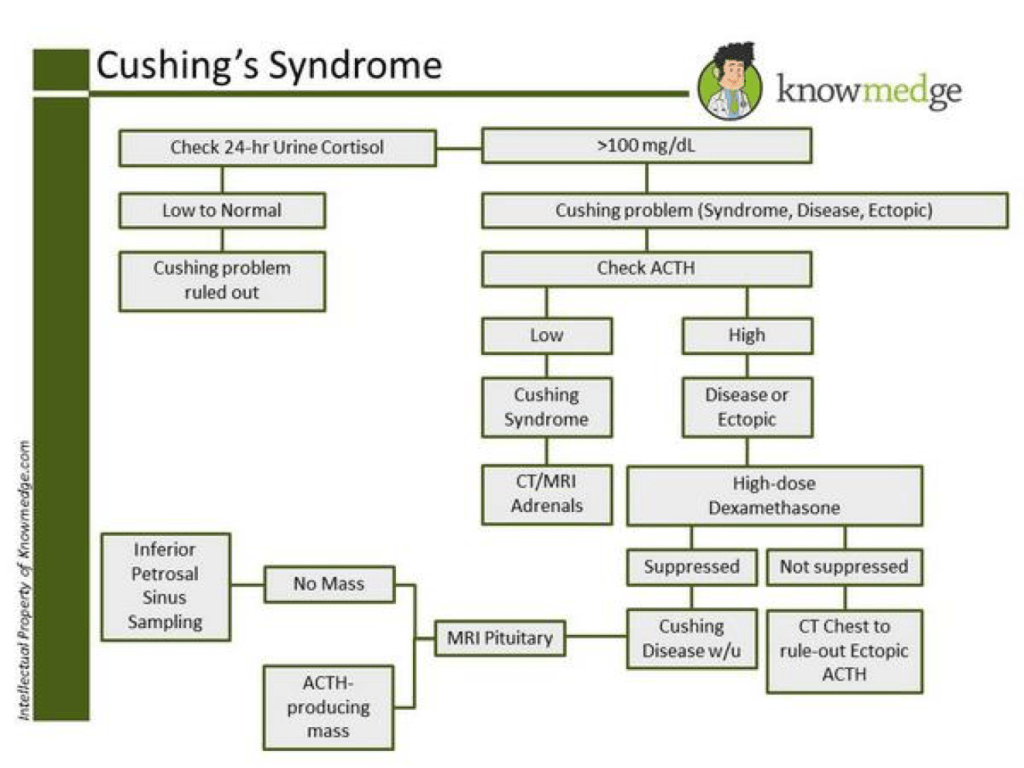
The initial SCREENING test of choice for Cushing Syndrome is a low-dose dexamethasone overnight suppression test. For this, 1mg dexamethasone is given around midnight and a serum cortisol is measured at 8am. A positive result is cortisol level of 1.8 mcg/dL.
The CONFIRMATORY test of choice for Cushing Syndrome is a 24-hour urinary cortisol excretion. A positive finding would be levels that are 3x the upper limit of normal for the assay used.
Once the diagnosis is made, the cause of the hypersecretion needs to be determined. For this, ordering a serum ACTH and high dose dexamethasone suppression test will help differentiate the various causes of the hypersecretion.
References
Findling JW, Raff H, Aron DC. The low-dose dexamethasone suppression test: a reevaluation in patients with Cushing’s syndrome. The Journal of clinical endocrinology and metabolism. 2004; 89(3):1222-6. [pubmed]
Dichek HL, Nieman LK, Oldfield EH, Pass HI, Malley JD, Cutler GB. A comparison of the standard high dose dexamethasone suppression test and the overnight 8-mg dexamethasone suppression test for the differential diagnosis of adrenocorticotropin-dependent Cushing’s syndrome. The Journal of clinical endocrinology and metabolism. 1994; 78(2):418-22. [pubmed]
Other Known Aliases – primary adrenal insufficiency
Definition – autoimmune destruction of the adrenal cortex that produces cortisol
Clinical Significance – In times of physiologic stress, the adrenal glands are unable to produce and secrete cortisol, which is a key hormone in the “fight-or-flight” response. If the stress is significant (trauma, surgery, hemorrhage, etc.), then the patient can not mount a compensatory response to this stress and can have life-threatening consequences.
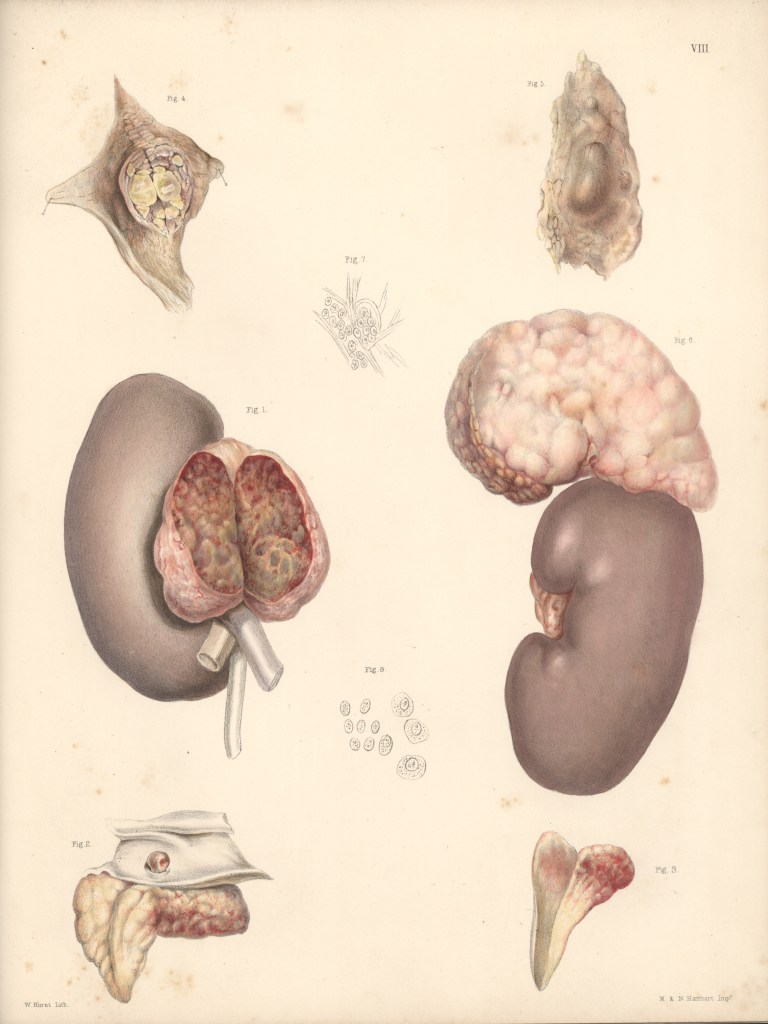
History – Named after Thomas Addison (1793-1860), an English physician who received his medical doctorate from the University of Edinburgh Medical School in 1815. He was a house physician at Guy’s Hospital and established himself as a prolific teacher and lecturer, often attracting physicians from all over London. He first described his eponymous disease in a short note in the London Medical Gazette called “Anaemia – Disease of the Suprarenal Capsules”. This was then followed up by the more well known article “On the Constitutional and Local Effects of Disease of the Suprarenal Capsule” in 1855, which is largely considered the beginning of the study of the adrenal glands. The disease eponym was original given to Dr. Addison by the French physician, Armand Trousseau, after fierce debate among experts as to whether the disease actually existed.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
47yo man presents to your clinic to establish care. He has a history of resistant hypertension, DMII, and sleep apnea. Vital signs are BP-159/101, HR-74, RR-16, O2-100%, and temp-98.9. Physical examination is also significant for multiple bruises on the lower extremities.
What would be the next step in the diagnosis of this patient?
What else would you need to order to determine the cause of this patient’s condition?
Definition – constellation of signs and symptoms due to excessive cortisol. This can be caused by several different mechanism that affect the hypothalamus-pituitary-adrenal axis:
CRH secretion by hypothalamus
ACTH secretion by:
Anterior pituitary
Ectopic tumor
Cortisol secretion adrenal glands by:
Adrenal hyperplasia
Adrenal tumor
Exogenous administration of corticosteroids
Clinical Significance – This is one of the more common endocrinologic pathologies you will see in clinical practice. Classic presentation includes obesity, abdominal striae, “moon face”, “buffalo hump”, and hirsutism. Diagnosis is made by obtaining a 24-hour urine cortisol measurement
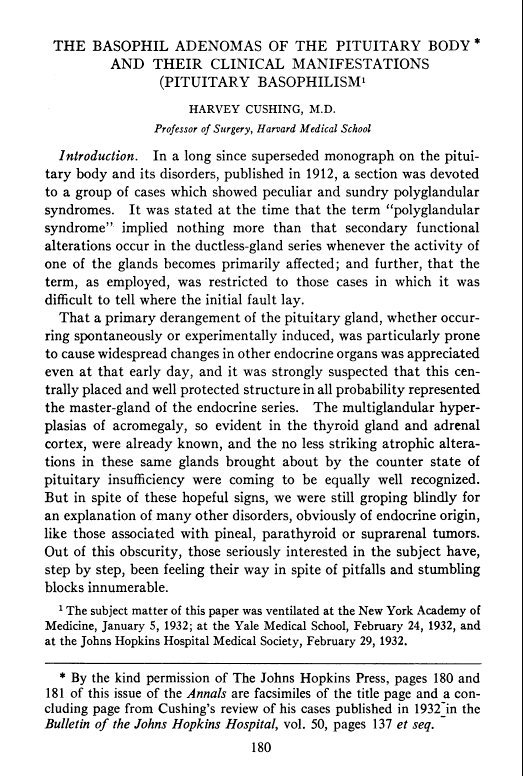
History – Named after Harvey Williams Cushing (1869-1939), who was an American surgeon and pioneering neurosurgeon of the early 20th century. He received his medical doctorate from Harvard Medical School in 1895. He completed his internship at Massachussets General Hospital and went on to do a surgical residency under William Halsted at John Hopkins Hospital. He trained under Kocher in England for several years before returning stateside and setting up practice in Baltimore. One of his greatest contributions to western medicine was his introduction of blood pressure management he learned from Scipione Riva-Rocci in Italy during his time in Europe.
At the age of 32, he achieved associate professor at Johns Hopkins Hospital and was placed in full charge of all surgery of the central nervous system. In 1912, he first described what would become his eponymous disease, but before he could publish it, he was called to serve during the first world war as the director for a field hospital in France for the British. It was during this appointment that he cared for a fatally wounded soldier by the name of Lt. Edward Revere Osler, son of William Osler. He formally published his findings on his eponymous disease in 1932 in an article entitled “The Basophil Adenoma of the Pituitary Body and Their Clinical Manifestations: Pituitary Basophilism”.
During his career, he was regarded as the world’s leading teacher of neurosurgeons for in the first decades of the 20th century and held professorships at Johns Hopkins Hospital, Brigham Hospital in Boston, Harvard Medical School, Yale School of Medicine, as well as honorary Fellowship in the Royal College of Surgeons. He also was awarded the 1926 Pulitzer Prize for Biography for his biography on the life of William Osler and was nominated for the Nobel Prize in Physiology or Medicine 28 times.
Cushing (far left) with Osler (second from right) and Kelley (second from left). Johns Hopkins Hospital. 1900.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
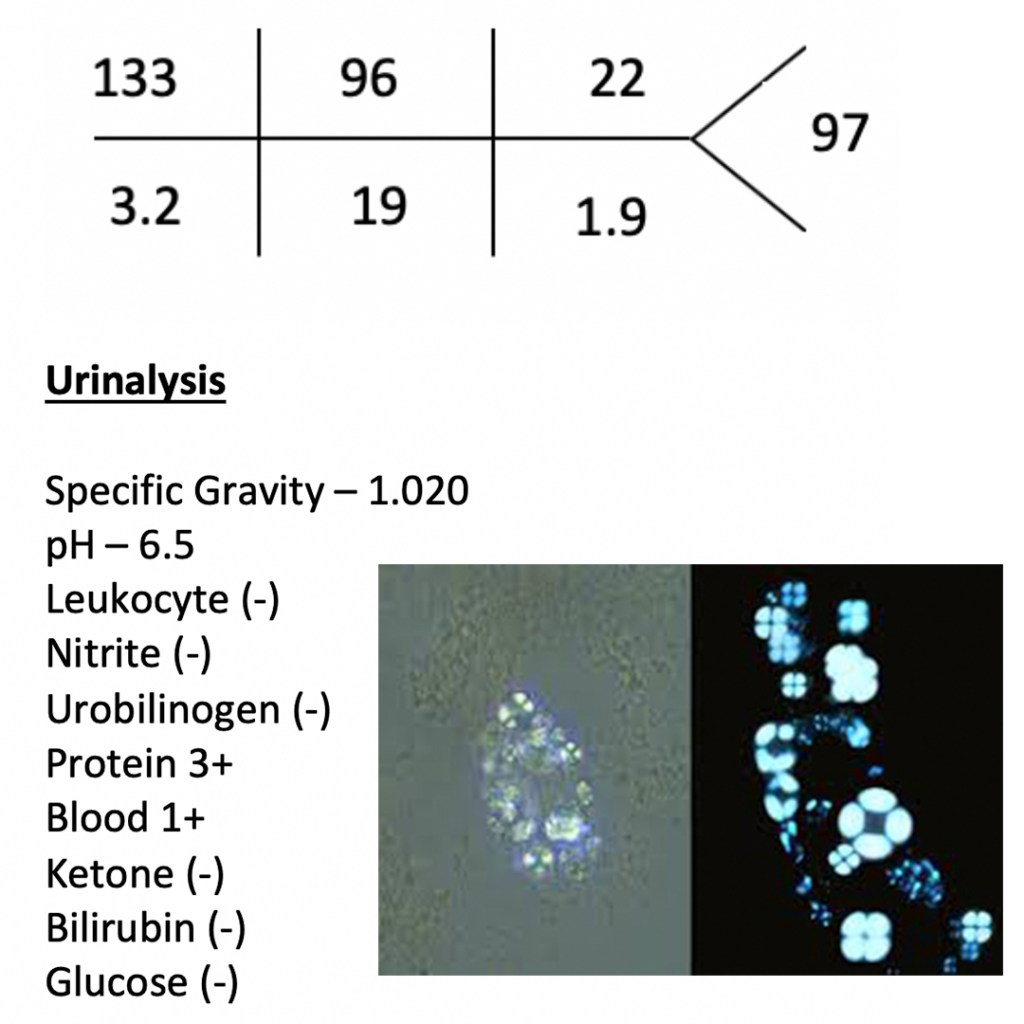
42yo woman, with a history systemic lupus erythematosus, presents to your clinic with a 1-month history of progressive leg swelling and polyuria. She is complaint with her medications and states that she hasn’t changed anything in her medical care. Physical examination reveals 2+ pitting edema to the knees in the lower extremities. BMP, UA, and urine microscopy are below.
What is the next step in diagnosing this patient and what would you expect to find?
Answer
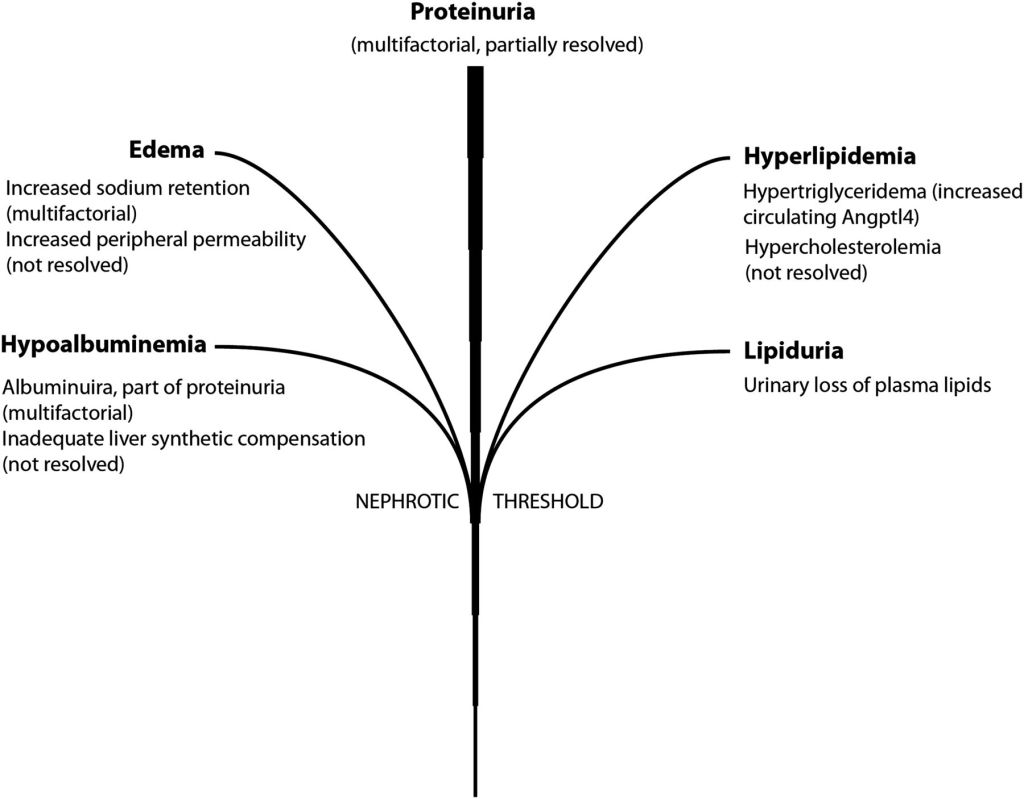
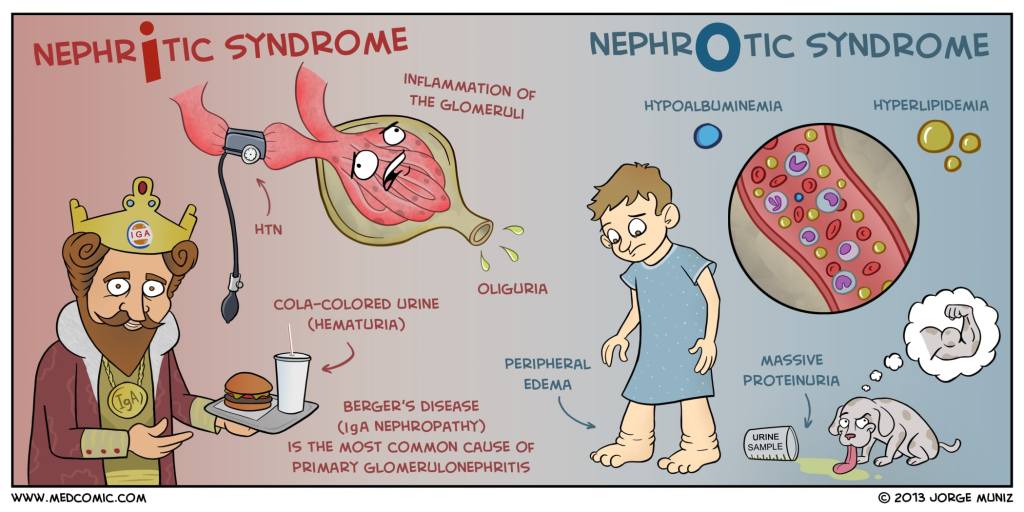
This patient found to heavy proteinuria on a urinalysis and oval fat bodies on urine microscopy, which would point to nephrotic syndrome as a diagnosis.
The next step in the diagnostic management of this patient would be to perform a 24-hour urine collection for urine protein. Normal urine protein excretion is < 150mg/day, but nephrotic range proteinuria is diagnostic at > 3.5g/day. Alternatively, a random urine protein-to-creatinine ratio of > 3.5 can be used, but is less reliable than a 24-hour collection.
Once a nephrotic syndrome diagnosis is made by urine studies, it should be followed up with a renal biopsy to determine the cause.
Group of disorders that cause a
metabolic acidosis due to defects in the renal tubules
Net retention of HCl
Net loss of NaHCO3
Pathophysiology
The kidney regulates acid-base balance two main ways:
Reabsorption of filtered HCO3
>80% of the bicarbonate filtered by the glomerulus is reabsorbed in the proximal renal tubules via Na-H exchange
Acid excretion
Collecting ducts of the nephron excrete hydrogen ions buffered by NH3 and PO3 (so the pH of the urine doesn’t destroy the nephron)
Extra production of NH3 is stimulated by intracellular acidosis.
3 step process
Reabsorption of sodium to create a negative gradient in the tubular lumen
Excretion of hydrogen by H-K-ATPase and reabsorption of potassium
Prevention of hydrogen ions from diffusing back out of the tubular lumen
Initial Presentation
Patients diagnosed with an RTA must first be diagnosed with a metabolic acidosis
Decreased pH with decreased HCO3
After this is determined, the anion gap must be calculated and found to be normal
AG = Na – (Cl + HCO3) = 8-12
Differential for NAGMA
Ureteric diversion
Small bowel fistulae
Excessive saline
Diarrhea
Carbonic anhydrase inhibitors
Renal tubular acidosis
Adrenal insufficiency
Pancreatic fistulae
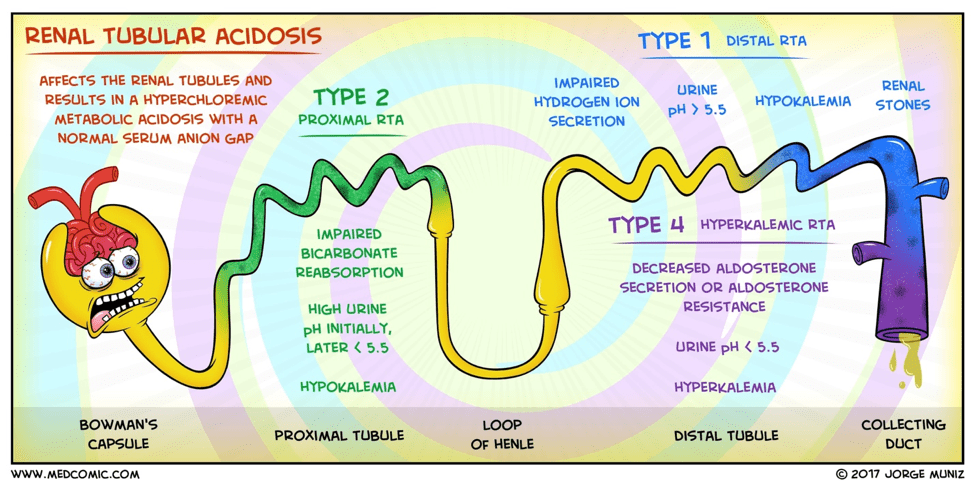
Type I (distal) RTA
Cause
Defect in the distal hydrogen ion
excretion
Pathophysiology
Failure of the H-ATPase proton pump
(most common cause)
Inability to acidify urine < 5.5
Hypokalemia
Increased hydrogen ion permeability
of the luminal membrane
Type II (proximal) RTA
Cause
Defect in proximal bicarbonate
reabsorption
Pathophysiology
Damage to the proximal tubule that
leads to progressive bicarbonate wasting in the urine
Type IV (hypoaldosteronism)
Cause
Reductions in aldosterone secretion
and responsiveness
Pathophysiology
Decreased rate of proton secretion
rather than an intrinsic defect in the tubule’s capacity to generate normal pH
gradient
Hyperkalemia causes reduced urine
NH4, which in turns leads to more acidic urine
Hydrogen ions have nothing to bind
to
Diagnostic Work-Up
RTAs should be considered in any
patient with a normal anion gap metabolic acidosis
Need ABG and BMP
Once this determination is made:
Urine pH
> 5.5 in type I (distal)
< 5.5 in type II (proximal) and
type IV
Urine ammonium
Elevated in type II (proximal)
Decreased in type I (distal) and
type IV
Most labs can’t measure urine
ammonium directly:
Urine Anion Gap (urine Na+K+Cl)
(+) UAG = > 20
Type I (distal) and type IV
(-) UAG = < – 20
Type II (proximal)
Serum potassium
Elevated in type IV
Decreased in type I and II
Treatment
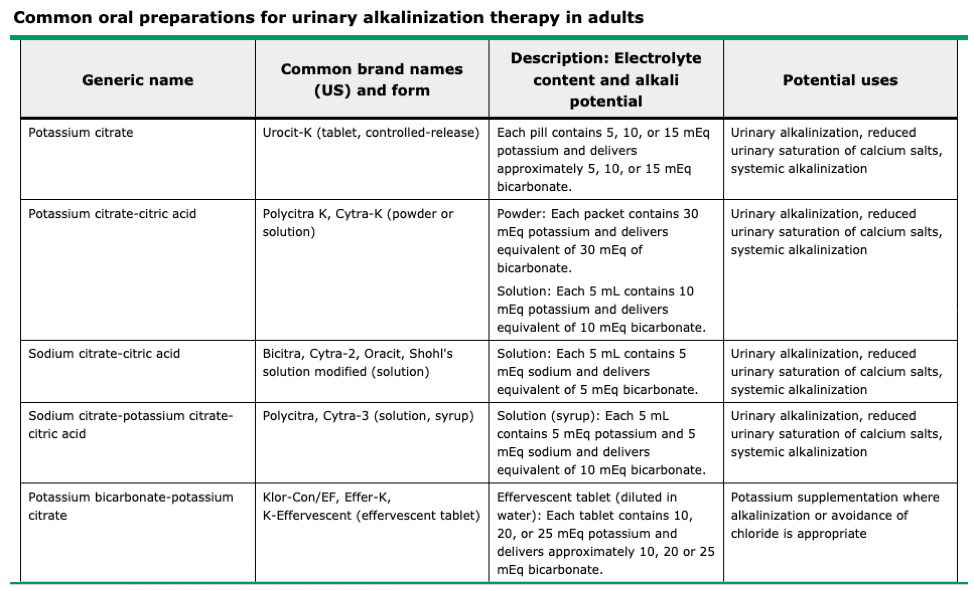
Type I (distal)
Urinarary Alkali Therapy
Sodium bicarbonate
Increased risk of nephrolithiasis due
to bicarbonaturia
Use potassium citrate instead
Type II (proximal)
Much more difficult to treat due to
the INCREASED bicarbonate diuresis during bicarbonate therapy
Alkali therapy (10x the dose for
type I) AND potassium salt repletion as bicarbonaturia INCREASES urinary
potassium losses
Thiazide diuretics if large alkali
doses ineffective or not tolerated
Diuresis reduces urinary bicarbonate
loss by increasing proximal sodium reabsorption
Which secondarily increased
bicarbonate reabsorption
Type IV
Stop any medication causes or treat
underlying condition (hypoaldosteronism)
Mineralcorticoid (fludrocortisone)
and glucocorticoid (hydrocortisone)
Potassium repletion
Up-To-Date. 2019
References
Rodríguez Soriano J. Renal tubular acidosis: the clinical entity. Journal of the American Society of Nephrology : JASN. 2002; 13(8):2160-70. [pubmed]
Skelton LA, Boron WF, Zhou Y. Acid-base transport by the renal proximal tubule. Journal of nephrology. ; 23 Suppl 16:S4-18. [pubmed]
Hamm LL, Nakhoul N, Hering-Smith KS. Acid-Base Homeostasis. Clinical journal of the American Society of Nephrology : CJASN. 2015; 10(12):2232-42. [pubmed]
42yo woman, with a history systemic lupus erythematosus, presents to your clinic with a 1-month history of progressive leg swelling and polyuria. She is complaint with her medications and states that she hasn’t changed anything in her medical care. Physical examination reveals 2+ pitting edema to the knees in the lower extremities. BMP, UA, and urine microscopy are below.
What is the next step in diagnosing this patient and what would you expect to find?
Definition – portion of the nephron that goes from the proximal convoluted tubule to the distal convoluted tubule. There are four portions of this structure:
Thin descending segment
Thin ascending segment
Ascending limb
Cortical thick ascending limp
Clinical Significance – the loop of Henle creates an area of high urea concentration with secretion and reabsorption of water and electrolytes. This is also the portion of the nephron where the aptly named “loop diuretics” to manage blood pressure by means of excess fluid excretion.
History – Named after Friedrich Gustav Jakob Henle (1809-1885), who was a German physician, pathologist, and anatomist and received his medical doctorate from the University of Bonn in 1832. He spent his early career as a prosector for Johannes Müller in Berlin where he published furiously on numerous facets of human and animal anatomy and physiology. He then went on to become the chair of anatomy at the University of Zurich, where he became one of the early adopters and advocates for the study of pathophysiology as a single distinct discipline. He also set the early argument for the germ theory in an essay entitled “On Miasma and Contagia”. His life’s work culminated in the publishing of the Handbook of Systematic Human Anatomy in 1855, which was the most complete and comprehensive work at that time.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.