
***LISTEN TO THE PODCAST HERE***
Background
- First described by Stein and Leventhal in 1935
- The most common cause of infertility in women
- Up to 30% of women seeking infertility treatment
- Affects 6-12% of US women ( or 1 in 10) of reproductive age
- Increases life-time risk of developing:
- Obesity
- DMII
- Cardiovascular disease
- Breast and endometrial cancers
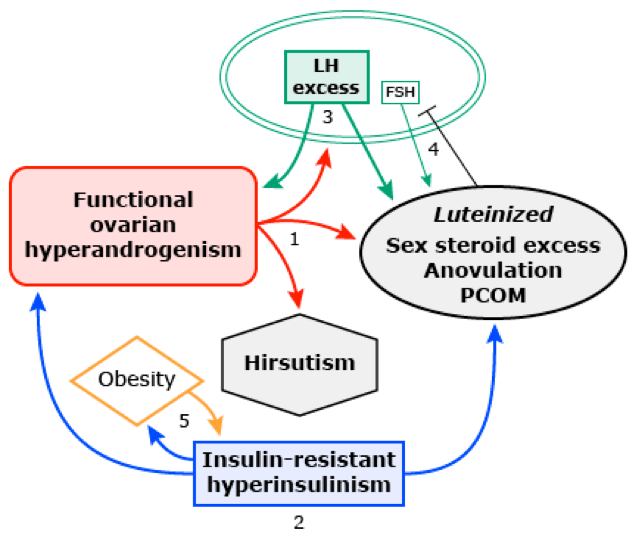
Pathophysiology
- Two-Hit Hypothesis
- First – genetic predisposition
- Heritable traits and gene variations affecting ovarian function, insulin resistance, obesity, and DMII
- 25% of patients with PCOS have a mother with PCOS
- Congenital virilization
- Congenital adrenal hyperplasia
- Disturbed fetal nutrition
- Heritable traits and gene variations affecting ovarian function, insulin resistance, obesity, and DMII
- Second – provocative trigger
- Insulin-resistant hyperinsulinemia
- Puberty
- First – genetic predisposition
- This then leads to the classic pathology of:
- Functional ovarian hyperandrogenism
- Hyperinsulinism and obesity
- Luteinizing hormone (LH) excess
Definition and Diagnostic Criteria
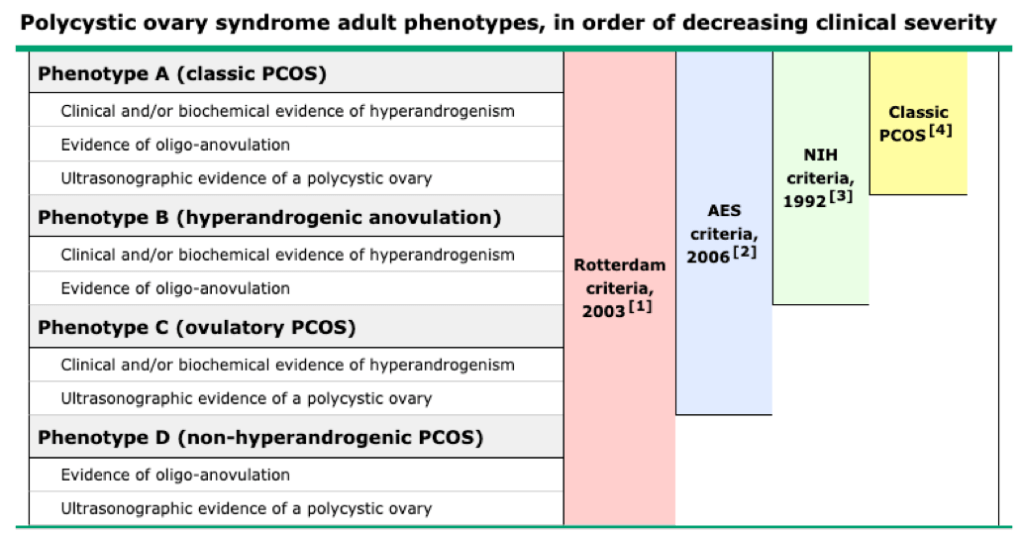
- Adults
- Rotterdam Criteria
- 2 of 3 following criteria:
- Anovulation
- Hyperandrogenism
- Polycystic ovaries
- 2 of 3 following criteria:
- Rotterdam Criteria
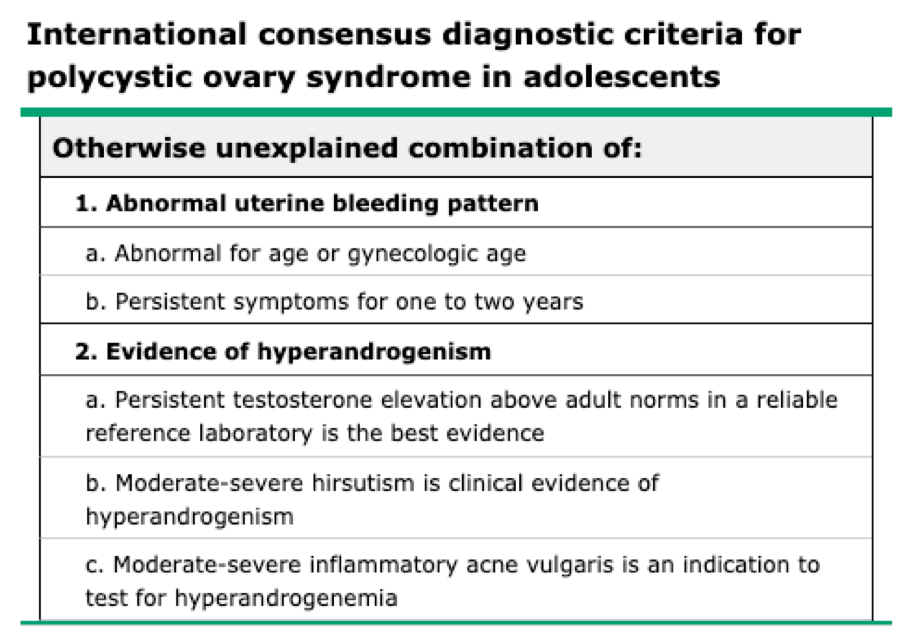
- Adolescents
- Developed in 2015 and consist of otherwise unexplained persistent hyperandrogenic oligo-anovulatory menstrual abnormality based on age and stage appropriate standards
Clinical Features
- Cutaneous Hyperandrogenism
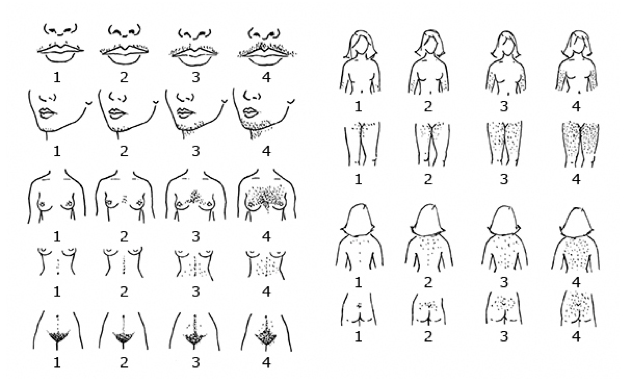
- Hirsutism
- Graded by Ferriman-Gallwey scoring system, which quantitates the extent of hair growth in androgen sensitive areas
- Hirsutism is defined as a score ≥ 8
- Graded by Ferriman-Gallwey scoring system, which quantitates the extent of hair growth in androgen sensitive areas
- Acne
- Moderate comedonal acne or severe inflammatory acne suggests hyperandrogenemia
- Hirsutism
- Ovarian Findings
- Menstrual
- Primary Amenorrhea
- Lack of menarch by 15 years of age or > 3 years after onset of breast development
- Secondary Amenorrhea
- > 90 days without a menstrual cycle after previously menstruating
- Oligomenorrhea
- During the first five years after menarache:
- Year 1 – < 4 cycles in the year
- Year 2 – < 6 cycles in the year
- Year 3-5 – < 8 cycles in the year
- Missing ≥ 4 cycles in the year
- Year 6+ – < 9 cycles in the year
- Missing ≥ 3 ycles in the year
- During the first five years after menarache:
- Excessive uterine bleeding
- More frequently than every 21 days or excessive bleeding
- PCOS is the most common cause of excessive uterine bleeding in adolescents
- More frequently than every 21 days or excessive bleeding
- Primary Amenorrhea
- Polycystic ovaries
- Menstrual
- Obesity
- Chief complaint in up to 20% of PCOS patients
- Sleep apnea or
- Nonalcoholic fatty liver
- Manifestations of insulin resistance
- Acanthosis nigricans
- Metabolic syndrome
- Up to 25% of PCOS patient

Diagnostic Work-Up
- Need to be performed at a lab with highly sensitive assay capability
- If using hormonal OCP, need to be stopped 2-3 months before testing
- Due to suppression of testosterone
- Testosterone (1st step)
- Should be early morning as testosterone levels fall by the afternoon
- Serum total testosterone
- Normal – 40-60 ng/dL
- > 150 ng/dL is diagnostic
- Serum free testosterone
- More sensitive than total, but are less standardized
- Only reliable if calculated from the total testosterone
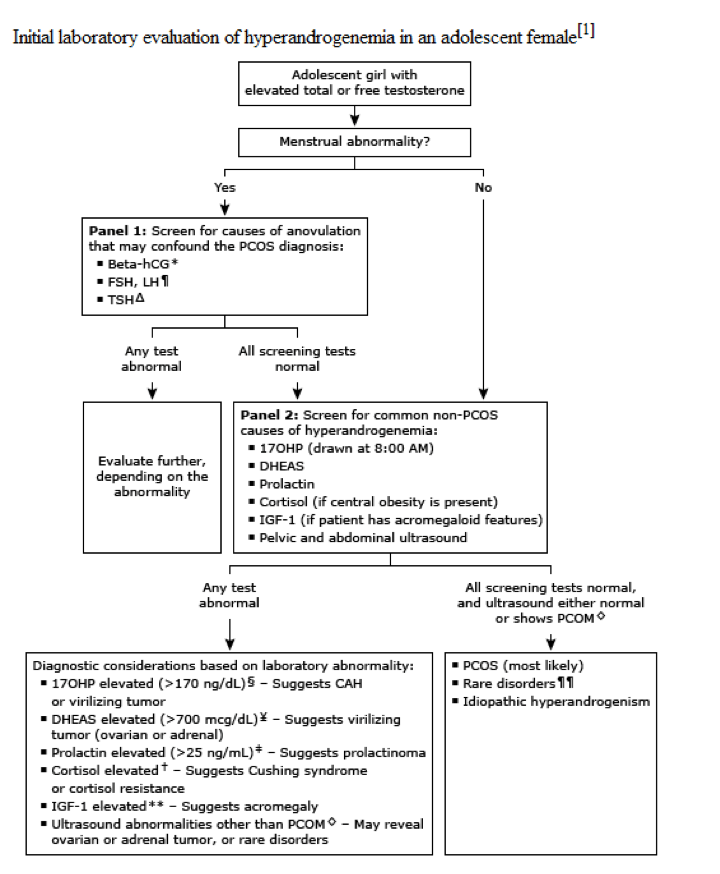
- Endocrine Screening Panel (2nd step if elevated testosterone)
- Beta-hCG
- FSH/LH
- Slightly elevated LH with a slightly decreased FSH is characteristic of PCOS
- Markedly elevated FSH = primary hypogonadism
- Markedly decreased LH = secondary hypogonadism
- TSH
- Screening for Common non-PCOS causes of hyperandrogenism (3rd step if endocrine screening is normal)
- 17-hydroxyprogesterone (17OHP)
- Drawn at 0800 and with the patient either amenorrheic or within the fist 10 days after the start of her menstrual cycle
- > 170 ng/dL suggests CAH
- DHEAS
- > 700 mcg/dL suggests adrenal tumor
- Prolactin
- Hyperprolactinemia can causes gonadotropin deficiency
- > 25 ng/m: suggests prolactinoma
- Serum cortisol
- < 10 mcg/dL rules out Cushing syndrome
- Insulin-like grown factor (IGF-1)
- Rule out acromegaly
- 17-hydroxyprogesterone (17OHP)
- Other tests
- Chronic disease panel
- CBC, ESR/CRP, CMP
- Lipid Panel (for adults)
- LDL, HDL, triglycerides
- Chronic disease panel
- Transvaginal ultrasound of ovaries
- Increased overall size
- Increased number of distinct follicles
- ≥ 6 is diagnostic

Treatment
- Adolescents
- Antiandrogen
- Estrogen-progestin combination OCPs
- Can also use GnRH agonist (leuprolide)
- Targeted antiandrogen therapy (if no improvement after 6 months)
- Spironolactone
- Finasteride
- Estrogen-progestin combination OCPs
- Insulin resistance
- Biguanide (metformin)
- Thiazolidinediones (pioglitazone, rosiglitazone)
- Antiandrogen
- Adults
- Same as above, but add:
- Dyslipidemia therapy
- Same as above, but add:
The Cottage Physician (1893)
References
- Stein IF, Leventhal ML. Amenorrhea associated with bilateral polycystic ovaries. AJOG. 1935;29(2):181-191 [article]
- Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO. The prevalence and features of the polycystic ovary syndrome in an unselected population. The Journal of clinical endocrinology and metabolism. 2004; 89(6):2745-9. [pubmed]
- Franks S, Stark J, Hardy K. Follicle dynamics and anovulation in polycystic ovary syndrome. Human reproduction update. ; 14(4):367-78. [pubmed]
- Barthelmess EK, Naz RK. Polycystic ovary syndrome: current status and future perspective. Frontiers in bioscience (Elite edition). 2014; 6:104-19. [pubmed]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertility and sterility. 2004; 81(1):19-25. [pubmed]
- Azziz R, Carmina E, Dewailly D, et al. The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report. Fertility and sterility. 2009; 91(2):456-88. [pubmed]
- Rosenfield RL. The Diagnosis of Polycystic Ovary Syndrome in Adolescents. Pediatrics. 2015; 136(6):1154-65. [pubmed]
- Witchel SF, Oberfield S, Rosenfield RL, et al. The Diagnosis of Polycystic Ovary Syndrome during Adolescence. Hormone research in paediatrics. 2015; [pubmed]
- Martin KA, Anderson RR, Chang RJ, et al. Evaluation and Treatment of Hirsutism in Premenopausal Women: An Endocrine Society Clinical Practice Guideline. The Journal of clinical endocrinology and metabolism. 2018; 103(4):1233-1257. [pubmed]
- Maslyanskaya S, Talib HJ, Northridge JL, Jacobs AM, Coble C, Coupey SM. Polycystic Ovary Syndrome: An Under-recognized Cause of Abnormal Uterine Bleeding in Adolescents Admitted to a Children’s Hospital. Journal of pediatric and adolescent gynecology. 2017; 30(3):349-355. [pubmed]
- Helvaci N, Karabulut E, Demir AU, Yildiz BO. Polycystic ovary syndrome and the risk of obstructive sleep apnea: a meta-analysis and review of the literature. Endocrine connections. 2017; 6(7):437-445. [pubmed]
- Elhassan YS, Idkowiak J, Smith K, et al. Causes, Patterns, and Severity of Androgen Excess in 1205 Consecutively Recruited Women. The Journal of clinical endocrinology and metabolism. 2018; 103(3):1214-1223. [pubmed]
- Pau CT, Keefe C, Duran J, Welt CK. Metformin improves glucose effectiveness, not insulin sensitivity: predicting treatment response in women with polycystic ovary syndrome in an open-label, interventional study. The Journal of clinical endocrinology and metabolism. 2014; 99(5):1870-8. [pubmed]
