

***LISTEN TO THE PODCAST HERE***
What are KDIGO and KDOQI???
- The 2 Organizations
- Kidney Disease Outcomes Quality Initiative (KDOQI)
- US Based
- Developed in 1997 by National Kidney Foundation
- Kidney Disease: Improving Global Outcomes (KDIGO)
- Global organization developing and implementing evidence based clinical practice guidelines in kidney diseases
- Developed in 2003 by NKF
- Essentially individual entities, but both comment various aspects of kidney diseases
- Kidney Disease Outcomes Quality Initiative (KDOQI)
- 2012 Guidelines
- Published by KDIGO and commented by KDOQI
- 5 chapters
Chapter 1: Definition and Classification of CKD
- Definition
- Abnormalities in kidney structure or function, present for > 3 months, with implications on health



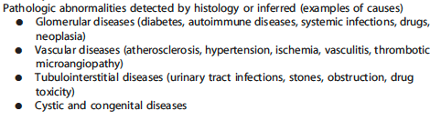
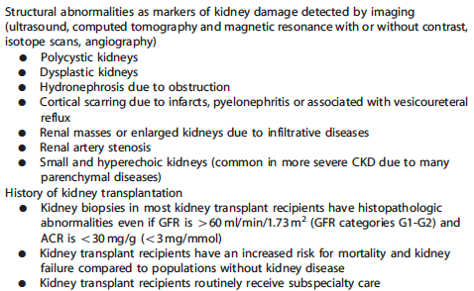
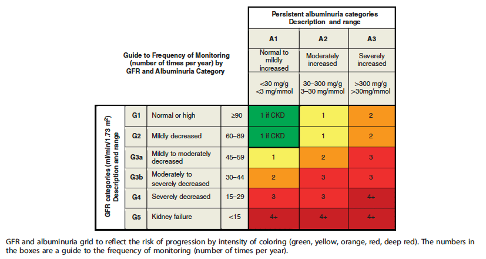
- Staging
- Based on causes, GFR category, and albuminuria category




- Predicting Prognosis of CKD

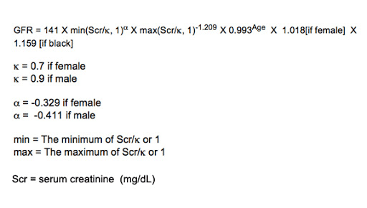
- Evaluation of GFR
- Recommend using serum creatinine and GFR estimating equation for initial assessment
- Recommend only using cystatin C in adult patients with decreased GFR but without markers of kidney damage if diagnosis of CKD is required
- Evaluation of Albuminuria
- Initial testing for proteinuria should be an early morning urine sample(in descending order of preference):
- Urine albumin-to-creatinine ratio (ACR)
- Urine protein-to-creatinine ratio (PCR)
- Reagent strip urinalysis for total protein with automated reading
- Reagent strip urinalysis for total protein with manual reading
- Microalbuminuria should no longer be used by laboratories
- If ACR > 30mg/g, then proceed to confirm with a random untimed urine sample
- Initial testing for proteinuria should be an early morning urine sample(in descending order of preference):
Chapter 2: Definition, Identification, and Predication of CKD Progression
- Assess albuminuria at least annually
- CKD progression is based on the one of the following:
- Decline in GFR category
- Drop in eGFR by ≥ 25% of baseline
- Sustained decline in eGFR by > 5mL/min/year
- Identify known risk factors associated with CKD progression
- Cause of CKD
- Age
- Gender
- Hypertension
- Hyperglycemia
- Dyslipidemia
- Smoking
- Obesity
- History of CVD
- Ongoing exposure to nephrotoxic agents
Chapter 3: Management of Progression and Complication of CKD
- Hypertension
- BP ≤ 140/90 if urine albumin excretion < 30mg/d
- BP ≤ 130/80 if urine albumin excretion > 30mg/d
- Recommend ACEI or ARB
- Protein Intake
- Recommend protein intake 0.8g/kg/d
- Glycemic Control
- Recommend HbA1C AROUND 7.0%
- ***newer ACE guidelines recommend < 6.5% with SGLT2i**

- Recommend < 2g/day
- Lifestyle
- Recommend 30 min/day five times per week, smoking cessation, and healthy weight (BMI 20-25)
- Lifestyle
- Complications Associated with CKD
- Anemia
- Diagnosed at < 13g/dL in men and < 12 g/dL in women
- Screening in patients with CKD:
- Stage G1-2 – when clinically indicated
- Stage 3a-3b – at least annually
- Stage 4-5 – at least twice per year
- Metabolic Bone Disease
- Obtained baseline calcium, phosphate, PTH, and ALP at least once in patients with GFR < 45 mL/min
- Not recommended to screen with bone mineral density testing
- Not recommended to supplement vitamin D of bisphophonates with deficiency or strong clinical rationale
- Acidosis
- Supplement oral bicarbonate in patients with serum bicarbonate < 22 mmol/L
- Anemia
Chapter 4: Other Complications of CKD
- CVD
- All CKD patients are at increased risk for CVD
- Recommend same testing and treating as non-CKD patients
- Use caution when interpreting NT-proBNP and troponins
- PVD
- Recommend regular podiatric assessment
- Medication Management
- Recommend using GFR for dosing adjustments
- Example – Metformin
- Stage G1-3a – continue
- Stage G3b – monitored
- Stage G4-5 – discontinued
- Example – Metformin
- Recommend using GFR for dosing adjustments

- Imaging studies and radiocontrast
- Avoid if possible, but do not hold if needed
- Following KDIGO Clinical Practice Guidelines for AKI
- Avoid high osmolar agents
- Use lowest contrast dose possible
- Stop nephrotoxic agents before and after
- Maintain adequate hydration
- Measure GFR 48-96 hours after
Chapter 5: Referral to Specialist and Models of Care



Cottage Physician (1893)

References
- KDIGO. Clinical Practice Guideline for the Evaluation and Management of CKD. 2012.
- Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014; 63(5):713-35. [pubmed]
- Stevens PE, Levin A. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013; 158(11):825-30. [pubmed]
- Andrassy KM. Comments on ‘KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease’. Kidney Int. 2013; 84(3):622-3. [pubmed]
